12. Laser Therapy
in Urology with Usage of Mustang 2000, Mulat-M10 Laser Devices
and
Mustang-VACUUM-DynaVac Vacuum Massage Device
M.L.Mufaged, L.P.Ivanchenko
Nonspecific inflammatory diseases of the
genitourinary system (GUS) organs are among the most common urological troubles
and come second to the acute respiratory diseases only for the frequency of
occurrence. According to the data from N.A. Lopatkin (1998), the infectious
inflammatory states in urology practices are found with very high frequency (up
to 78%). Unfortunately, main group of population suffering from these diseases
are young people of child producing age, the peak of diseases falls within the
age of 26–41
years.
There are primary inflammatory affections of
various GUS parts: pyelonephritis, cystitis, prostatitis, epididymo-orchitis,
and secondary processes, which develop in connection with the diseases of other
organs and systems. Also, complications after various operative and
instrumental interventions occur. The nonspecific inflammatory processes in GUS
having an iatrogenic genesis are worthy of special attention because a
successful control of them influence pronouncedly both, the quality of living
of the diseased people and the level of medical treatment of the population as
a whole.
Conventionally applied treatment modalities of
inflammatory diseases of kidneys, urinary tract and male genital organs not
always satisfy the clinicians with their results. Insufficient effectiveness of
treatment employing the routine methods is caused most commonly by a range of
factors:
• impaired circulation in an affected organ;
• innervation disorder (of functional nature);
• impairment of bioavailability of organs for antibacterial and
anti-inflammatory medicines.
These factors are connected with a variety of
causes, main of which are: oedema of affected organ tissue, suppression of
microcirculation in the region of inflammation and presence of various
barriers. All this drives to look for the new ways of solution of this issue by
making use of the present-days achievements of science and technology.
Low-level laser therapy (LLLT) is one of such innovative methods of medical
treatment, which is increasingly applied in urology practices from year to year
and open up the new opportunities and prospects in treatment of GUS
inflammatory diseases.
We examine in this paper certain proprietary
treatment techniques of a wide range of urologic diseases of inflammatory
genesis. Each of these diseases and methods of laser therapy has its
particularities, which are set out in the following sections.
Often, sexual disorders are connected with
chronic infectious diseases of genitourinary sphere both, indirectly and
directly. Therefore, we do not specify this section in a separate chapter and
just point up additionally an emotional and psychological side of solution of
this issue.
Before the reader becomes familiar with the
material presented therein, we draw particular attention to some critical
points:
• magneto-laser therapy of GUS inflammatory diseases may be applied
as a sole treatment in very rare cases only, but most often as
a part of a
multimodality therapy;
• patients with kidney diseases must undergo any treatment at
in-patient facilities only and under the control of specialists;
• laser therapy should be accompanied with intake of
antioxidants.
1. Amyloidosis
Amyloidosis is a complex anomaly of protein
and carbohydrate metabolism, which results in formation of a special substance
– amyloid fibrous protein,
in the internal organs and systems. Nowadays, there is found out the
heterogeneity of amyloid fibrils which localize perireticularly or around
collagenous fibres that is accompanied with dysfunction of certain organs:
kidneys, lungs, heart etc.
The preventive measures are focused largely
on the secondary amyloidosis and are aimed at the control of infections. Within
the period of sufficient renal function the patients should take adequate
nutrition with moderate restriction of cooking salt if any oedema. In case of
renal insufficiency the treatment modality shall be changed depending on
intensity of clinical signs.
Application of intravenous laser blood
irradiation (ILBI) in the course of treatment of AA-amyloidosis in the patients
with rheumatoid arthritis (RA) using the method described below in the course
of routine treatment methods showed better results.
Laser therapy (LT) technique: intravenous laser blood irradiation
(ILBI) using Mulat-M10
laser therapeutic device (Fig. 1), optical radiation
power at the light-guiding fiber output 1.5–2.0 mW, 10–12 daily sessions, duration of a
session 25-30 minutes.

Fig. 1. Mulat-M10 laser therapeutic
device
Repeated course of laser therapy in 6 and 12
months. Then the courses of laser therapy are repeated every 12 months during
not less than 5 years when possible.
2. Sterility
According to the contemporary literature, up
to 12–15% of married
couples are sterile, including through the husband’s “fault” in 40–45% of the cases [Kamalov A.A., 2000;
Tarasov N.I. at al., 1999]. In the general structure of the male sterility
causes the existing inflammatory diseases of genital organs come steady second
– third that made it
possible to classify a separate form of sterility – excretory toxical [Yunda I.F., 1990],
or excretory inflammable [Guidance on Andrology, 1990].
Conventional medication therapy in case of
chronic inflammatory diseases of the reproductive system organs though not
always normalizes the fertility that makes the researchers look for
alternative, in particular, drug-free modalities of male sterility. They
include also magneto-laser therapy (MLT). The available medical books present
single statements of local MLT application in spermatogenesis pathology, which
is usually of complementary nature and prescribed along with the medication or
at the final stage of conventional treatment [Avdoshyn V.P. at al.,
1994].
Meanwhile, it has been known that LLLT, both,
continuous red (0.65 µm), and pulse IR (0.89 µm), in vivo, and in
vitro, makes a stimulation effect on the sperm
– the energetic processes
are improved. Moreover, exposure to pulse IR-irradiation is more effective at
the optimum exposure time of 5 minutes [Goryunov S.V., 1996].
Researches by V.V. Yurshyn (2003) proved that
increase of sex and gonadotrophic hormones content in the blood serum of the
patients having excretory inflammatory form of sterility is observed at the
time when MLT is applied with its peak in the middle of 10-day course of
treatment. The level of lactotropic hormone is conversely reduced within the
same time period, and the tendency for normalization of all indices is observed
in a month.
In V.V. Yurshyn’s opinion (2003), differences in directional orientation of
response of gonadotrophic and lactotropic hormones of hypophysis are caused by
MLT’s action not directly
on hypophysis, but through the hypothalamus, wherein the products of
gonadoliberin realising factor and prolactin inhibiting factor are
“coupled” causing, in turn, an increase in secretion of
follicle-stimulating and intestinal cell-stimulating hormones while prolactin
hormone formation is inhibited. Increase of the level of reproductive hormones
is connected with both, hypophyseal stimulation of endocrine function of
testes, and reflex action on genital glands through the vegetal nervous system
(VNS); moreover, MLT promotes the line “intestinal cell-stimulating hormone
– testicular hormone”,
and it should be applied in asthenozoospermia and oligospermia with pronounced
sperm motility impairment.
The pregnancy incident of wives of these
patients was 41.7 and 55.4% respectively, and they gave birth in 35.8 and 49.7%
of the cases. In the course of the given treatment of patients with excretory
inflammable form of sterility using MLT, a positive therapeutic effect was
achieved in 95% of the cases, remission of more than 1 year was observed in 85%
of the examined patients [Yurshyn V.V., 2003].
Other researches also speak about promising
outlooks of LLLT in the complex treatment of patients suffering from secretory
sterility. Thus, it was demonstrated that the sperm motility (a + b) is truly
increased after LLLT exposure from 17 to 29% (р = 0.0002 – by sign test), number of
morphologically normal forms from 25 to 35% (р = 0.0001 – by sign test), number of viable sperm
from 60 to 66% (р = 0.04 –
by sign test).An analysis of the hormonal panel showed the tendencies for
reduction of follicle-stimulating hormone (FSH) level in the patients suffering
from the pronounced oligoasthenoteratozoospermia from 11.5 mIU/ml to 8.0 mIU/ml
(р = 0.05 – by sign test,
р = 0.09 – by the
Student’s coefficient) that
is indicative proximately of LLLT effect on the Sertoli’s cells [Mazo E.B. et al., 2002;
Mufaged M.L. et al., 2004].
LT technique: transcutaneous contact MLT using
Mustang 2000 or Mustang 2000+ laser therapeutic device
(Fig. 2). LO4-2000 laser
radiation probe (Fig. 3) with ZM50 magnetic attachment (50 mT) (Fig. 4),
output radiation power 10–15 W, frequency 80 Hz.

Fig. 2. Laser therapeutic device (basic unit)
of Mustang 2000+ series

Fig. 3. Appearance of laser radiation probes
of pulse radiation

Fig. 4. ZM50 magnetic attachment
Exposure of testicles to bipolar laser
radiation is carried out in succession within 5 min. for each testicle, and
then within 2 min. within the area of edgebone and perineum. The course
consists of 10 daily sessions.
3. Glomerulonephritis
Glomerulonephritis (GN) is a kidney
inflammatory disease of immune genesis with the primary and major affection of
glomeruli, as well as with involvement of other structural elements of renal
tissue into pathological process; has a steadily progressing course with
outcome into chronic renal insufficiency (CRI). The glomerulonephritis is
subdivided into immunoinflammatory nephritis (membranoprofilerative
glomerulonephritis and mesangiocapillary glomerulonephritis) and
non-inflammatory nephropathies (membranous glomerulonephritis, focal segmental
glomerulosclerosis).
Treatment of the patients suffering from GN
is rather difficult and complicated task. Main task of the treatment is
confined to inhibition of immunoreactions by cytostatic and/or
glycocosticosteroid agents. In case of GN, the possibility of absolute recovery
is in in doubt, and if it happens, it is just in single cases. Oftener, it is
possible to reach more or less full or partial remission of different duration.
Therefore, the primary aim in GN treatment is to slowdown the rate of the
disease progression and to prevent the course of chronic renal insufficiency,
to get the remission (clinical or clinic-laboratorial) as long as possible and
to maintain the patients’
capacity to work and quality of living for an extended period. The treatment of
the patients with GN should be complex and include prescription of a regime, which corresponds to the
state of the patient and course of disease, various health aids, reasonable
diet therapy and sanatorium-resort methods if possible.
Improvement in the patients’ health status suffering from
glomerulonephritis after application of LLLT consists in normalization of the
state of health, blood pressure stabilization, improvement of the functional
renal tests, decreased activity of inflammatory process with development of
clinic-laboratorial remission, reduced proteinuria, increased diuresis
[Greenstein Yu.I., 1995; Sleptsova T.G. et al., 1995].
In view of stages and elements of the
glomerulonephritis pathogenesis, it can be assumed that these benefits in the
treatment of glomerulonephritis using LLLT come thanks to induction of
catalase, superoxide dismutase (SDM) ferment strength, which abrogate the
pronounced lipid peroxidation in the form of reduction of intermediate products
of lipid peroxidation (diene conjugates and malondialdehyde). The cholesterin
quantity
and content of free membrane fatty acids in
the lymphocyte membranes in the patients suffering from glomerulonephritis are
truly increased, and the quantity of general lipids, cholesterin, and
triglycerides is reduced in the blood serum. Moreover, the repair of
rheological disorders occurs as a result of true reduction of erythrocyte
deformability [Greenstein Yu.I., 1995].
Protracted application of LLLT has a positive
effect on hemodynamic regardless of the clinical variant of glomerulonephritis
process – promoting
transition of hyperkinetic and hypokinetic types of the blood circulation into
normokinetic. Because of the fact that forecasting unfavourable types of blood
circulation occur oftener at the mixed clinical variant of progress and
nephrotic syndrome, the percentage of transition is more than in the patients
suffering from the isolated urinary syndrome [Lutoshkin M.B.,
2003].
Laser therapy is indicated by the method of
intravenous laser blood irradiation. ILBI is accompanied by a pronounced
positive effect on the basic clinical presentations of hypertensive syndrome
against reduction of arterial blood pressure that makes it possible to cancel
the intake of specific antihypertensive drugs for more than one fourth of the
patients, and for other patients – to reduce the basic antihypertensive therapy by more than twice,
in so doing to decrease the quantity of the medications taken and to make the
treatment cheaper. Taking into account some tensity of antioxidant protection
system in the patient’s
organism suffering from GN, antioxidants are prescribed for the patients. Most
commonly, it is Polyoxidonium at the dose of 6 mg daily.
LT technique: ILBI using Mulat-M10 laser
therapeutic device, continuous radiation wavelength 0.65 µm, optical radiation
power at the light-guiding fiber output 1.5–2.0 mW, duration of a session 30 to 45
minutes. Treatment course consists of 10–12 sessions. Repeated courses in 3, 6,
9 months to consolidate the treatment achievements or for preventive
reasons.
4. Diabetic nephropathy
It is generally thought that hyperfiltration
and intraglomerular hypertension underlie the progression of both, non-diabetic
and diabetic renal insufficiency. Moreover, in case of diabetes, common
multisystemic, inclusive of renal, polyneural angiopathy occurs, which results,
in turn, in impairment of blood circulation in kidney parenchyma. The
angiotensin-converting enzyme inhibitors and natural antioxidant and
aneoprotector α-lipoic acid
are considered to be well-established medicaments for treatment of this
dangerous complication. The improvement rate of the indices and their further
maintenance at the achieved level after implementation of these groups of
medicaments is better in the patients which treatment is carried out on the
back of laser therapy.
Laser therapy is
carried out in accordance with a complex method as a part of a multimodality
therapy.
Technique 1: ILBI using
Mulat-M10 laser therapeutic device. The first 5 sessions are carried out by
intravenous blood irradiation within 25–30 minutes with optical radiation power at the light-guiding fiber
output 1.5–2.0 mW,
wavelength 0.65 µm. In the course of ultra-violet irradiation (UVI) of blood
the exposure time 5–7 min.,
radiation power 1 mW, wavelength 365 nm (Mustang
2000 or Mustang
2000+ laser therapeutic device, VLOK-LED-365 laser radiation probe (Fig. 5)).
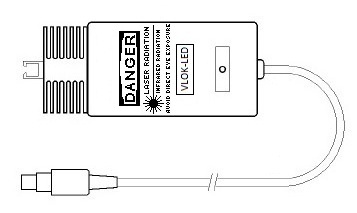
Fig. 5. Appearance of VLOK-LED-365
light-emitting diode radiation probe
Technique 2: transcutaneous contact MLT using
Mustang 2000 or Mustang 2000+ laser therapeutic device. The following
5–7 sessions. There is
carried out an exposure of kidney projections to radiation symmetrically by
pulse IR-laser probe of MLO1K-2000 matrix type (wavelength 0.89 µm) (Fig.
6) with MM50 magnetic attachment (50 mT) (Fig. 7), pulse recurrence frequency 80
Hz, output radiation power 40–50 W within 1.5–2 min. per zone. Decades-long researches showed that the pulsed
laser radiation of red spectrum – LOK2-2000
laser radiation probe, makes more effective an action
on the vascular system (Fig. 3), output radiation power 3 W, wavelength
0.63–0.65 µm also within
1.5–2 min. per zone
(Mustang 2000 or Mustang 2000+ laser therapeutic device).

Fig. 6. Appearance of MLO1K-2000 laser
radiation probe of matrix type
I. View of display panel. II. View of window
for radiation outlet.

Fig. 7. MM50 magnetic attachment
The repeated courses are carried out in 3 and
6 months. During the following 5-10 years a course of laser therapy must be
carried out once per year.
All the patients receive a complex therapy
for underlying disease, pancreatic diabetes, with consideration of type,
variant and severity level of the underlying disease.
The LT sessions carried out improve the
quality of the patients’
living by reducing, mitigating the intensity of the clinical presentations of
uremic intoxication and the pancreatic diabetes itself – polyneuropathy, angiopathy, skin itch,
dyspeptic disorders. The data available are eloquent of general positive effect
of LLLT on the kidney function state in the patients suffering from pancreatic
diabetes in the event of development of diabetic nephropathy [Lutoshkin M.B.,
2003].
5. “Steinstrasse” after extracorporeal shock wave
lithotripsy
Large-scale implementation of the method of
extracorporeal shock wave lithotripsy of kidney and ureter calculi in the
clinical practice has aggravated a problem of prevention of ureteral occlusion
by small fragments of destroyed calculi and the relevant complications. The new
technical capabilities in the field of extracorporeal shock wave lithotripsy
make it possible to destroy the calculi completely in 90–95% of the cases. However, the major
problem lies in evacuation of the destroyed calculus fragments from different
parts of ureter. Despite the fact that in most cases the size of the fragments
of the destroyed calculus in the form of “steinstrasse” is not more than
2–3 cm, weeks and sometimes
months are required for their passage. Unfortunately, the currently used
methods of non-operative, medicamental, physiotherapeutic action on a calculus
or destroyed calculus fragments not always result in achievement of the desired
effect. That is exactly why application of LT, taking into account its
pathogenetic capabilities (antiedematous, analgesic, enhancing the
contractility of ureter wall action etc.) is justified in treatment of this
category of the patients [Alekseev A.V. et al., 2002].
It was discovered the stimulating effect of
LLLT on the urodynamic of the upper urinary tract, change in amplitude and
frequency of peristalsis. The therapy by pulsed IR laser radiation appeared to
be the most effective, makes it possible to vary the parameters of effect
[Safarov R.M. et al., 1996].
V.P. Avdoshyn (2000) has suggested a
technique which lies in combination of conventional treatment modalities
(spasmolysants, uroseptics, urinative herbs, medications of terpenes group)
with carrying out of LT. It is used pulsed IR radiation (laser probe of
LO4-2000 type), output radiation power 4–7 W, pulse recurrence frequency
1000–1500 Hz, using
scanning technique, no less than on 3 zones: 1st zone – projection of ureter below the
localization of “steinstrasse”, 2nd projection – projection of “steinstrasse”,
3rd – kidney protection by two fields on the
side of affection. Duration of a session - 5–10 min. for each zone. LT sessions are
carried out until removal of “steinstrasse” from the urinary
tract.
Other data evidences the pronounced
therapeutic effect of MLT on the process of passage of calculus fragments
from the urinary tract after extracorporeal shock wave lithotripsy
compared with conventionally used treatment methods (medicamental and
physiotherapeutic). The usage of MLO1K-2000 matrix pulsed laser radiation
probe with MM50 magnetic
attachment appeared to be the most effective [Khalyastova E.A et al.,
2002].
Technique: contact transcutaneous MLT using
Mustang 2000 or Mustang 2000+ laser therapeutic device. MLO1K-2000 laser radiation probe with MM50 magnetic
attachment (50 mT), maximum output radiation power 50–80 W, pulse recurrence frequency
1000–1500 Hz. The first day
– an action on projection
of calculus or “steinstrasse” and on projection of ureter segment located
below the calculus; 2nd day
– action by MLT on the same
point and on the kidney projection; 3rd and following days – action by MLT on all 3 fields. Time of exposure on each point
– 5 min. The course
consists of 8–10 daily
sessions. All patients are treated with spasmolytic, analgesic and antibiotic
drugs to prevent the development of inflammatory complications [Khalyastova
E.A. et al., 2002].
6. Magneto-laser therapy under hemodialysis, after kidney
transplantation
The patients on hemodialysis or after kidney
transplantation suffer often from various complications and critical
conditions, in which it is not always useful or it has no sense to apply
already known treatment techniques or modalities for various
reasons.
In the first place, this is progression of
cardiovascular insufficiency in the form of ischemic heart disease, myocardial
infarct, pericarditis, arterial hypertension etc. Septic and cerebrovascular
complications are the next. Haemorrhages of different localization may cause
fatal cases of the patients that are promoted by application of large doses of
heparin during the session. Moreover, the disease process and blood
transfusions carried out result in growth of pre-existing antibodies in the
patients’ organisms, and
their high titre makes it impossible to perform a life and death surgery
intervention –
transplantation of kidney.
It is well known that the hyperkinetic
variant of heart insufficiency is developed in most patients receiving
treatment by program hemodialysis. Application of cardiac glycosides is not
recommended under such conditions since it may contribute to further
progression of circulatory insufficiency. Therefore, there is a necessity of
further study of the new alternative approaches and techniques of cardiac
insufficiency correction in such patients [Lutoshkin M.B., 2003].
Laser therapy of the patients with terminal
renal insufficiency receiving the treatment by program hemodialysis
results in decrease of development of complications by 55–60%, reduction in total peripheral
resistance and improvement of cardiac function, positive reduction of the level
of triglycerides, pre-beta-lipoproteids, cholesterin, normalization of lipid
peroxidation processes, improvement of activity indices of oxidation
– reduction processes,
improvement of microcirculation connected with dilation of capillaries and
improvement of rheological blood values based on the coagulogram data. It is
noted smoother course of uremic pericarditis and decreased lethality, shortened
periods of disease in case of suppurative-septic complications, their
resolution passed faster than in the control group due to reduced endogenous
intoxication (the level of urea, creatinine, medium molecules), as well as
elimination of immunological paralysis condition after pronounced
immunodepressive therapy carried out in connection with the transplanted kidney
rejection episodes [Zakharov V.V. et al., 1995; Lebedkov E.V., 1995; Sernyak
P.S. et al., 1995].
After ILBI a true reducing of subjective and
objective signs of cardiac insufficiency is noted on average in the whole group
of the patients examined. A true tendency for decreased laboured breathing,
fatigability, orthopnoea is identified. The severity of cardiac insufficiency
as per classification of the New-York Cardiological Society is decreased from
3.4 ± 0.3 to 2.8 ± 0.31 class (р < 0.05). All examined patients have
increased myocardial contractility by 6.4% (р < 0.05) with the concurrent
contraction of the left ventricle: end-diastolic volume (EDV) – by 5.8% (р < 0.05), end-systolic
volume (ESV) – by 6.5% (р
< 0.05). In the course of dynamic study of the microcirculatory bloodstream
condition, reduction in perivascular oedema, regeneration of arterial and
venular bypasses, increase of blood velocity is observed. Identification rate
of sludge-syndrome was reduced from 92 to 45%, arterial-venular index has
increased from 0.18 ± 0.01 to 0.32 ± 0.017 (р < 0.05) [Lutoshkin M.B.,
2003].
Technique: ILBI by means of Mulat-M10 laser
therapeutic device. Optical radiation power at the light-guiding fiber output
2.5–3.0 mW, wavelength 0.65
µm, duration of a session 50–60 minutes, 10 sessions per treatment course.
7. Urolithiasis
We have used three principal directions in
approach to the issue of therapy using MLT in treatment of urolithiasis (ULT):
treatment of ULT itself (litholysis), lithokinesis and lithiasis.
The patients with urolithiasis are the most
frequent patients of urological clinics – up to 40% of the total number of
urological patients. The application of extracorporeal shockwave lithotripsy in
the therapy of the patients with urolithiasis makes it possible often to solve
the problem, but a range of complications are possible (renal colic,
aggravation of an urinary infection, obstruction of the upper urinary tract
with the fragments of destroyed calculus, with development of acute obstructive
pyelonephritis).
Owing to main therapeutic features of LLLT,
its application is the most effective in combination with the conventional
treatment methods of patients with renal colic. Such technique makes it
possible to accelerate rapid relief of renal colic symptoms, to increase the
intervals between the episodes. Passage of calculi on the background of such
therapy goes often painless [Avdoshyn V.P., 2000].
The laser therapy in case of renal colic is
carried out in the scanning mode on the projection zones of ureter below the
calculus localization, calculus projection, and kidney projection by two
fields. Pulse IR-radiation probe (LO4-2000 type), pulse recurrence
frequency 1000 Hz, pulse radiation power 5–7 W, duration of one session 5 min. on
each zone. LT sessions are carried out daily until the calculus went out of the
urinary tract [Avdoshyn V.P., 2000].
Application of magneto-laser therapy for the
patients with urate nephrolithiasis is justified in connection with the
stabilizing effect on the membranes resulting in normalization of colloid
systems. The normalization of uric acid indices in the blood serum and in urine
is reached on the 5th day of
therapy. V.P. Avdoshyn et al. (2001) showed conclusively that application of
MLT in a complex therapy aimed at prevention of the secondary prophylaxis of
lithiasis is pathogenically substantiated and reasonable. According to Kh.F.
Lakhlu (2001), application of MLT in a complex treatment and prevention of a
disease makes it possible to prevent calculus formation in the patients with
urate nephrolithiasis in 96.6% of the cases and in the patients with oxalate
nephrolithiasis in 100% of the cases.
Technique 1: transcutaneous contact MLT using
Mustang 2000 or Mustang 2000+ laser therapeutic devices. Within preoperative stage. Two radiation
probes of LO4-2000 type with
ZM50 magnetic attachments, frequency 1500–3000 Hz, pulse radiation power
8–12 W. Transcutaneous
contact-mirror action (Fig. 8) parasternally (zone 1) at the level of the
second intercostal space, then on inguinal vascular fascicles (zone 4) within 2
min. on each, and on projection zone of calculus front and rear (zones 2, 3)
within 4 min. on each – radiation probes shall be moved slowly down within the zone of
12–15 cm length. Action is
repeated in 4–6 h. In many
cases, the magneto-laser therapy carried out according to this scheme against
increased fluids and medication (spasmolytic, analgesic drugs etc.), promotes
passage of calculi and cancellation of surgery.

Fig. 8. Magnetic laser therapy technique in
urolithiasis
Technique 2: transcutaneous contact MLT using
Mustang 2000 or Mustang 2000+ laser therapeutic device. After the calculi have been passed (or in
postoperative period) the magneto-laser therapy is carried out on a daily basis
within 5–7 days
1–2 times per day. Action
is made on the area of affected kidney (zone 3) and on inguinal vascular
fascicles (zone 4) within 2 min. on zone. MLO1K-2000 matrix pulse IR-radiation
probe with MM50 magnetic
attachment, output radiation power 40–50 W, pulse recurrence frequency 600–1000 Hz.
8. Acute pyelonephritis
In addition to the general principles of
acute pyelonephritis treatment when selecting MLT therapy technique, a
pathogenic factor which caused the development of disease is of paramount
importance. According to the conventional classification the following
pathogenic ways of infectious agent penetration into a kidney are
distinguished: hematogenic, ascending urinogenic and ascending along the ureter
wall. Thus, for instance, in case of hematogenic way of infection penetration,
pockets of infection in the organism shall undergo magneto-laser treatment. In
case of the urinogenic way the treatment using ILBI and magnetic therapy (MT)
of infectious diseases of small pelvis organs should be provided. In case of
ascending along the ureter wall type of spread of infection it is necessary to
apply the technique described in section related to the treatment of chronic
interstitial cystitis. Transcutaneous LT is indicated for treatment of all
types of acute pyelonephritis for the purpose of improving the microcirculation
in parenchyma of the affected kidney; intravenous laser blood irradiation
– in case of pronounced
depression of cell- and antibody-mediated immunity; a combined technique - in
case of any suppurative-septic diseases of kidneys with pronounced
intoxication.
According to V.P. Avdoshyn et al. (2005),
after carrying out magneto-laser therapy in complex treatment of acute
pyelonephritis in main group, the normalization of indices of physical,
laboratory and ultra-sound testing occurs at an earlier date that in the
control group. In main group (as against of control one) a tendency for
normalization of ELI-P-test-1 values is observed. Moreover, the repeated
attacks of acute pyelonephritis during this pregnancy and after delivery were
noted more rarely among the patients of main group, premature births were
observed more rarely. Moreover, they delivered the babies with better
characteristics as per Apgar scale and with higher body weight compared with
the babies delivered by females of the control group. Application of MLT in the
complex treatment of acute pyelonephritis within the 2nd half of pregnancy is effective not
only in the treatment of the disease itself, but also it decreases the
probability of the repeated pyelonephritis attacks during the pregnancy and
after delivery, as well as it makes it possible to improve the forecast
regarding the physical condition of the new born.
Technique 1: transcutaneous contact MLT using
Mustang 2000 or Mustang 2000+ laser therapeutic device. Exposure of kidney projection to
MLO1K-2000 laser probe with
MM50 magnetic attachment,
output radiation power 40–50 W, frequency 3000 Hz, in sequence within 4–5 min. per zone. Number of sessions -
not more than 10, daily or every second day.
Technique 2: ILBI using Mulat-M10 laser
therapeutic device, wavelength 0.65 µm; radiation power 1.5–2 mW within 10–20 min., 7–10 sessions on a daily basis or every
second day. Ultraviolet irradiation (UVI) of blood: exposure time 3–5 min., radiation power 1 mW,
wavelength 365 nm (Mustang 2000 or Mustang
2000+ laser therapeutic
device, VLOK-LED-365
radiation probe).
9. Acute and chronic cystitis
Cystitis is an inflammation of urinary
bladder. The disease is of frequent occurrence among women of childbearing age.
Introduction of infection occurs by ascending tract along the lumen of urethra;
moreover, bigger danger of cystitis occurrence for women is determined by
anatomic topography features of genitourinary tract structure: short urethra,
close anatomical position of sheath and fundament to the external urethral
opening, structure features of Lieutaud body epithelial layers, urethra and
vaginal opening, as well as high occurrence rate of inflammatory diseases of
genital organs. These factors create favourable conditions for localization and
spread of continuously vegetating microflora into one of the organs of
genitourinary tract and conversion of the process into chronic form of
disease.
Acute cystitis is a
disease with the most frequent occurrence in everyday medical practice,
especially in outpatient conditions. The diagnostics of acute cystitis creates,
as a rule, no problem for any doctor. The treatment includes prescription of
antimicrobial medicines, dietary intervention with exception of spicy and
irritating food. A pronounced therapeutic effect is observed if LT is included
in a set of curative measures, which may be started since the patient seeks
medical advice [Avdoshyn V.P., 2000].
The laser therapy is carried out
simultaneously by means of MLO1K-2000 pulse IR-matrix radiation probe and LO4-2000, by pairs, on the projection
area of urinary bladder (zone 6), on LV acantha (zone 4), kidneys (zone 2), inguinal vascular fascicles
(zone 5) and zones 1 and 3 (Fig. 9). Pulse recurrence frequency 80 Hz, exposure
time 1.5–2 min., radiation
power 60 and 7 W respectively, number of sessions – not less than 5. As a general rule,
already after the second-third session the patient’s urination is normalized, dysuria
disappears.
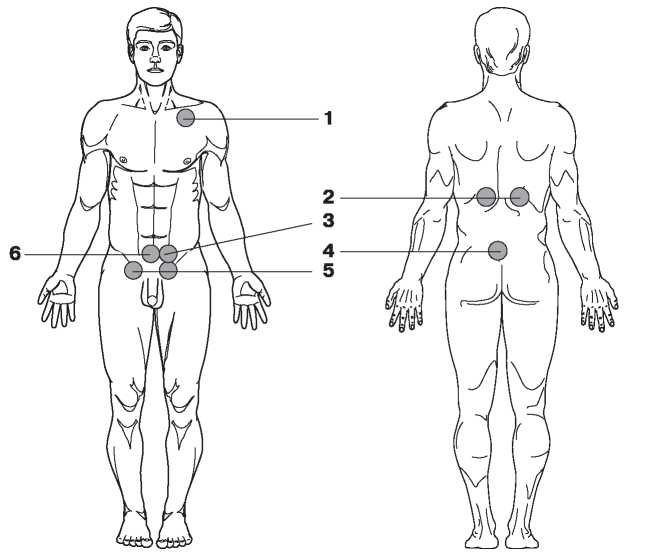
Fig. 9. Magneto-laser therapy technique if
cystitis
If acute cystitis is accompanied by
inflammatory diseases of genital organs, consecutive irradiation of urinary
bladder projection and uterine appendages using MLO1K-2000 laser probe (with the same
parameters) is carried out or irradiation of urinary bladder projection using
LO4-2000 laser probe and
simultaneous, using the same probe with vaginal attachment of type G-1 (Fig. 10) for Mustang 2000 or Mustang 2000+ laser therapeutic device. Exposure time – 5 min. on each area, number of
sessions – not less than
7.

Fig. 10. G-1 vaginal attachment
Chronic cystitis requires longer-term treatment which should include, in addition to
the conventional antimicrobial therapy, a intravesicular installations of
various antiseptic medicines (silver preparations, Dibunolum, Synthomycin
emulsion etc.) into urinary bladder. LT is carried out by means of placing
emitter on the urocyst projection in suprapabic area. Exposure time - 5 min.,
pulse recurrence frequency 80 Hz – the first 3 sessions and sessions 7–10, frequency 3000 Hz – sessions 4–6. In specific situations, LT course
may be repeated independently (with no other kinds of treatment) in 10 days
after completion of the first course. The efficiency is evaluated by the status
of the patient, as well as based on the data of the clinical laboratory
indices.
10. Acute epididymo-orchitis
Acute inflammation of appendage – acute epididymitis (AE), is one of
urological diseases of the most frequent occurrence developing both,
independently, and in combination with acute inflammatory process in testicle
– epididymo-orchitis (AEO).
More than 25% of middle-age and young men have suffered from this disease in
the course of their lifetime.
In the modern medicine, the application of
ILBI as one of the methods of physical action on various organs gained a wide
popularity. The reason for this is that exactly ILBI has a pronounced
anti-inflammatory and analgesic effect, improves general and local immunity,
and improves the microcirculation in the area of inflammation influencing the
penetrance of vessel walls. The most important feature of laser therapy is the
fact that an effect of photo activation of biological and physiological
processes in the whole organism is initiated at the local exposure.
An adequate detection of topical forms of the
disease is crucial for application of differentiated disease management. In an
equivalent manner it is important both, theoretically and practically,
distinguishing of AE and AEO at the stage of infectious inflammatory process.
For the time being, unfortunately, there is practically no standard
classification of AE and AEO, which could be used by doctors in their daily
work. Based on the peculiarities of clinical laboratory and sonographic changes
in the appendages and testicles in case of AE and AEO, in M.L.
Mufaged’s opinion (1995),
it is reasonable to use a classification, which includes 4 stages:
• serous;
• suppurative-infiltrative;
• fine-focal suppurative-destructive;
• macrofocal (abscessed) suppurative-destructive.
It has been established that AE and AEO stage
is associated, as a general rule, with remoteness of the disease in the absence
of an adequate therapy. If the remoteness of disease is about 3 days, the stage
I of AE develops only, if the remoteness of disease is within 5 days
– stage II. If the
remoteness of disease is more than 5 days, AE of the stage III develops, if
more than 7 days – stage
IV. The AE course depends also on kind and virulence of its invader, the
immunity status of the patient’s organism as a whole.
AE and AEO diagnostic methods and
magneto-laser therapy efficiency control are subdivided into 3 basic groups:
clinical, laboratory and ultrasound methods of examination.
The clinical methods of examination include
interview and study of complaints and anamnesis of the patients, examination
and palpation of marsupium organs, digital rectal investigation of prostate
gland.
The laboratory examination consists of
clinical blood analysis, prostatic secretion analysis (PCR to detect any
urogenital infection), urine and ejaculate culture, immunology research as the
acute infectious inflammatory processes within the area of marsupium, and in
all other organs result in significant immunological deviances in the organism
which are classified as the category of the secondary
immunodeficiency.
Particular importance should be paid to the
ultrasound investigation as the most objective and informative method of AE and
AEO diagnostic and control of the therapy efficiency in the course of
treatment. Ultrasound investigation only is capable to detect truly not only
the topic form (AE or AEO, primary affection of this or that segment of
testicle or its appendage), but the stage of the disease, too. In the course of
ultrasound investigation it is necessary to assess the size, shapes, and
sharpness of contours, echostructure of testicles and epididymis, the presence
of space-occupying masses, destructive changes and degree of their extension,
as well as the presence of liquid in the marsupium cavity. In the serous stage
a uniform decrease of echo-density is detected, in the diffuse – suppurative stage – its uniform increase, and in case of
fine-focal– and macrofocal
destruction – the relevant
areas of increase and decrease of echo-density. U/S-monitoring makes it
possible to adjust and optimize MLT doses and modes in the course of its
application [Mufaged M.L., 1995].
Efficiency control of the therapy conducted
is performed by method of ultrasound monitoring every three days from the
beginning of the delivery of therapy. In the initial stages (I– II) of acute epididymitis without
signs of the process spread on any testicle, it is recommended to continue the
local magneto-laser therapy after relief of the most acute signs under
outpatient treatment under medical supervision by an urologist at place of
residence and U/S-monitoring until absolute recovery. In the stage IV of AEO
(macrofocal suppurative-destructive) the only surgical treatment is
recommended.
Laser therapy is
recommended to conduct depending on the stage and topical form of the disease
[Local Laser Magnetic Therapy…, 2002].
In the stage I of AE (serous) MLT is applied mainly independently. Mustang 2000 or Mustang
2000+ laser therapeutic
device. Transcutaneous laser irradiation of testis, epididymis of testis is
performed by contact method, stationary. The recommended course – 7–10 sessions. Sessions are to be
conducted on a daily basis, once per day. Radiation frequency for pulse lasers
1500 and 3000 Hz in biosynchronized mode (BIO controller
is connected (Fig. 11), heart rate and respiration sensors are on the patient),
exposure time on one field – 5 min.

Fig. 11. BIO controller for Mustang 2000 laser
therapeutic device
Emitters location as in Fig. 12:
• LO4-2000 laser
radiation probe, output radiation power 7–10 W, with ZM50 magnetic
attachment (50 mT) – on
projection of the
upper pole of testis;
• Simultaneously, KLO3-2000 laser radiation probe (Fig. 13), maximum output radiation
power, with ZM50
magnetic attachment
(50 mT) – on projection of the lower pole of
testis.

Fig. 12. Magneto-laser therapy technique of AE
in stage I (serous)

Fig. 13. Appearance of laser and
light-emitting diode radiation probes of continuous radiation mode
(completed with additional button switch of
modulation mode)
Direction of radiation probes – crossed. The irradiation is conducted
in within the area of projection of the head (upper pole of testis) and tail
(upper pole of testis) of epididymis. Location of emitters in red and infrared
spectral bands may be changed depending on localization of the epididymis
affected area with consideration of crossed direction of the
emitters’ action. However,
the radiation probe in red spectrum should be directed directly on the
epididymis affected area. Position of the patient – lying flat on back, on treatment
couch, with legs spread. In case of one-side process, the first 5 sessions
shall be conducted on the side of affection localization, the following
2–5 sessions – on both sides simultaneously. In case
of two-sided process, irradiation is conducted on both halves of marsupium
– bilateral in the same
mode.
In the stage II of AE (diffuse,
suppurative-infiltrative) magneto-laser therapy is
applied in combination with an antibacterial treatment (broad spectrum
antibiotics). Transcutaneous laser irradiation of testis, epididymis of testis
is performed by contact method, stationary. Recommended course – 10–12 sessions. The sessions are conducted
on a daily basis, once per day. Pulse recurrence frequency for pulse lasers
1500 and 3000 Hz in biosynchronized mode, total exposure time – 10 min. Location of laser radiation
probes as Fig. 14:
• KLO3-2000 laser radiation probe with
ZM50 magnetic attachment (50 mT) on projection of the upper pole of the
first testicle,
maximum output radiation power (8–10 mW);
• Simultaneously, LO4-2000 laser radiation probe, output radiation
power 7–10 W, with
ZM50 magnetic attachment (50 mT) on
projection of upper pole of the
second testicle toward KLO3-2000;
• MLO1K-2000 matrix radiation probe, output radiation power 50–60 W, on projection of lower poles of
both testicles.

Fig. 14. Magneto-laser therapy technique of AE
in stage II (diffuse, suppurative-infiltrative)
Position of the patient – lying flat on back, on treatment
couch, with legs spread.
In the stage III of AE or AEO (fine-focal
suppurative-destructive) magneto-laser therapy is
applied in combination with an antibacterial treatment (broad spectrum
antibiotics). Transcutaneous laser irradiation of testicles, epididymis of
testicles is performed by contact method, stationary. Recommended course
– 10–15 sessions. Sessions shall be
conducted on a daily basis, 2 times per day with interval between the sessions
5–6 hours. Pulse recurrence
frequency for pulse lasers 3000 Hz in biosynchronized mode, total exposure time
– 10 min. per one session.
Emitters’ location in the
1st session as in Fig.
15:
• LO4-2000 laser radiation probes (output
radiation power 7–10 W) and
KLO3-2000 (maximum output
radiation power) with ZM50
magnetic attachments (50 mT) on projection of the upper half of marsupium
(upper poles of both testicles);
• LO4-2000 laser radiation probes (output
radiation power 7–10 W) and
KLO3-2000 (maximum output
radiation power) with ZM50
magnetic attachments (50 mT) on projection of the lower half of marsupium
(lower poles of both testicles).
The position of probes in red and infrared
spectra alternates every other day.

Fig. 15. Magneto-laser therapy technique of AE
in stage III (fine-focal suppurative-destructive),
1st session
Location of radiation probes in the
2nd session as shown in Fig.
16:
• MLO1K-2000 matrix radiation probe, power
50–60 W horizontally on
projection of one testicle;
• MLO1K-2000 matrix radiation probe, power
50–60 W vertically on
projection of other testicle.
Position of the patient – lying flat on back, on treatment
couch, with legs spread.
If the therapy conducted is not effective,
surgical treatment is required.
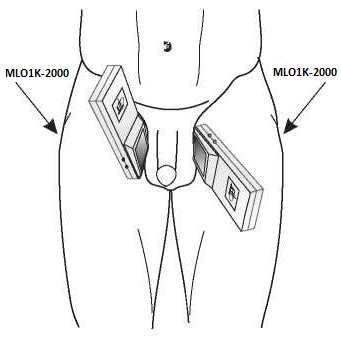
Fig. 16. Magneto-laser therapy technique of AE
in stage III (fine-focal suppurative-destructive),
2nd session
11. Incisions
Laser therapy is an effective technique of
treatment of patients, who underwent various operative interventions, repair
and reconstructive operations on ureter, operations for ureter- and
vesicovaginal fistulas, plastic operations for enuresis. Application of the
technique makes it possible to reduce the time of regenerative processes, to
reduce the likelihood of complications occurrence.
LT technique: stationary, distant. Treatment sessions
are conducted the day before the operation and in 2–3 days after. LO4-2000 radiation probe, pulse radiation power 7–10 W or MLO1K-2000, pulse radiation power
40–50 W (Mustang 2000 or
Mustang 2000+ laser therapeutic device), frequency 80 Hz. Action within the area
of an incision in 2-3 zones within 0.5–1 min. per zone. The course may be repeated in 4-5 days if
necessary.
12. Prostatitis
Inflammatory affections of prostate gland,
seminal vesicles, seminal hillock (prostatitis,
vesiculitis, colliculitis) are the most common
diseases of the genitourinary sphere of men taking often a chronic course. The
prostatitis is subdivided into bacterial and abacterial. This classification
approach will be important for selection of one or another treatment technique.
In case of bacterial prostatitis, a “banal” or nonspecific flora is
detected in secretion of prostate gland. In case of abacterial prostatitis,
intracellular activators (STD) whether can be detected in the secretion of the
prostate gland and in the scrape from urethra, or they can be not present
therein.
The mechanism of disease progression is
rather complicated. Most often, several factors should be present
simultaneously: anatomic and functional disturbances in prostate (as a
consequence of acute prostatitis suffered earlier or an attach of chronic
prostatitis with cicatrical-sclerotic outcome), venal and lymphatic stasis
within the pelvic organs, immunodifficient conditions (of both, local and
general genesis), the presence of an infectious agent of various aetiology,
disorders in the part of urination (ureter-prostatic reflux), sex life rhythm
disorders etc.
The following presentations come to the
foreground in clinical progression of the prostatitis: dusyric and pain
syndromes, sexual frustrations, reproductive changes and psychoneurological
syndromes. Therefore, the prostatitis is not only a medical, but also a social
problem in view of age of the patients and prevalence of the
disease.
The prostatitis has got a status of a
separate disease entity more than 100 years ago. An advanced chronic
inflammatory process in man’s genitals, as a general rule, is widespread, but a driving or main
abnormal focus is located in one organ only.
Congenital
pathogenetic or contributory causes of pathology development in the prostate
gland include the following:
1) anatomic and physiological features of
the prostate gland: crypto shaped mucous coat of excretory ducts of
acini-glandules; it causes hindered outflow of its secretion due to changes in
viscosity and pH value, on one hand, and due to compression of excretory ducts
by oedema, on the other hand, hampers the effectiveness of
medication;
2) congenital absence of compressors,
muscles bracing and compressing the excretory duct openings, prostate
gland lobes which are opened on the rear wall of posterior urethra (contributes
to introduction of infection due to retrogradely occurring urethra-prostatic
reflux);
3) disturbance of arterial blood supply to
the prostate gland promoting tissue hypoxia occurrence; in the course of a
treatment it hampers the possibility of adequate transportation of
antimicrobial and antiviral medications to the target organ;
4) abundance of anastomoses among the
prostate gland venae and pelvis low tension circulation contributes to
spreading of pelvic congestions (congestive occurrences) into this organ that
has an adverse effect not only on the run of the inflammatory process, but also
on copulative and reproductive sexual functions (as well as arterial blood
supply insufficiency);
5) anatomical vicinity of sex accessory
organs (prostate gland, seminal vesicles, seminal hillock) causes a mutual
ingress of infection that gives grounds for application of therapy by physical
factors with the whole set of diseases of genitourinary sphere, including
posterior urethritis, in mind;
6) anatomical vicinity of rectum causes the
lymphogenic infection contamination of the prostate tissue with underlying
congestion and disturbed arterial blood flow into the prostate gland
tissues.
Among the acquired pathogenetic factors the
immunologic one deserves special attention.
The pre-existing factors can be classified
into the following basic groups in order of significance:
1) causing the development of congestion
(stasis) in the small pelvis organs;
2) potential pockets of
infection;
3) depressing the testosterone metabolism
and causing the androgen deficiency;
4) promoting vegeto-neurotic disorders in
the pelvis organs;
5) weakening general and local immunological
responses.
The mechanism of action of contributory
causes may be two-way. In some cases, the protective responses in the prostate
gland are weakened (congestion in the pelvis organs, androgen deficiency,
vegeto-neurotic disorders, changes in acid-base potential toward alkaline side,
weakening of general and local responsiveness), in other cases, the potential
disturbing factors (genital-pelvic) and extragenital pockets of infection and
metabolic correlative factors are brought to the forefront. The potential
disturbing factors include obligate (infectious agents) and facultative (immune
alterations, androgenic disturbances, vegetovascular changes).
The secretion of prostate gland has
antibacterial properties. Weakening or loss of these properties can be caused
by: androgen deficiency of testicles due to acquired diseases or congestive
effects; change in the secretion pH values. Account must be taken of functional
condition of the accessory sexual glands. Particularly, acid-base potential is
of great importance.
Disorders of pelvic blood circulation
promote the development of inflammatory process in the prostate gland. Because
the powerful parasympathetic ganglia and abundant network of sympathetic
receptors are located in the prostate gland and within the pelvic area, the
disorders of the vegetal nervous system conditions can be their cause (primary,
etiological) rather than the consequence of organic changes in the prostate
gland (secondary, pathogenetic). In the first case, the therapy should be
started with repair of VNS disorders, and in the second case, the prostatitis
should be treated in due time. VNS disorders disappear with resolution of
infection in the prostate gland.
In case of any chronic intoxications
(tabaccoism, alcoholism etc.), pancreatic diabetes, trauma, exposure of
ionizing irradiation, nervous-vegetal, vascular and immune disorders as a
result of their long-term indirect action on the prostate gland,
disruption of trophism, vegetal innervations, and immune responsiveness of the
gland occurs. Occurring thereby the destructive degenerative-trophic changes
promote the conversion of non-pathogenic and potentially pathogenic flora into
pathogenic (the quantitative factor has a paramount importance) causing the
occurrence of an inflammatory process. Resulting from a wide and, over all,
uncontrolled application of strong antimicrobial medications the potentially
pathogenic flora penetrating deeply into the organs of urogenital system causes
a chronic inflammatory process. Fungus diseases are thereat of frequent
occurrence.
Spread of pathogenic flora from remote
organs (tonsillitis, caries, influenza, respiratory diseases etc.) occurs by
hematogenic way in 3–12% of
the cases. Lymphogenic spread of infection into the prostate gland is observed
if any inflammatory focus is present in neighbouring and subjacent organs
(rectum, urinary bladder, bulbourethral glands, testis, and seminal vesicles)
in 8–17% of the cases.
According to different authors, urethral or canalicular way of infection
contamination composes 75–100%. According to I.F. Yund (1981), urethritis and urethral way of
infection contamination is possible as a result of action of the preceding
factors which cause dysbacteriosis, weakening of inter-organ protective
mechanisms and subsequent introduction of infection.
The degree of a pathologic process spread
depends on the disease remoteness and way of the infection contamination. In
case of hematogenic and lymphogenic ingress of infection the inflammatory
process is often acute and localized. Urethrogenic and canalicular
contamination of infection results, as a general rule, in involvement of a
number of organs, the inflammation presents less acutely. Both variants of the
inflammation course are united by commonness of the preceding factors. The
success of therapy depends largely on their timely repair.
Clinic-bacteriological examinations of the patients with inflammatory diseases of male
genital organs (orchitis, epididymitis, epididymo-orchitis, funiculitis,
vesiculitis, prostatitis, colliculitis, posterior urethritis, balanitis,
balanoposthitis) with the use of a separate single-step getting of excretes of
genital organs (secretion of prostate gland, secretion of seminal
vesicles, ejaculate, urine) gave interesting results: non-identical microscopic
flora was found in 34.5% of the patients. This goes to prove that the
inflammatory diseases of genital organs of the same patient may be caused by
both, common and different causative agents that is important to take into
account when prescribing the medicaments.
In case of latent
prostatitis, the inflammatory focuses are located
usually near the urethral tract. Microscopically, the gland is not changed,
though the inflammatory elements may be found in its secretion. In case of
calculary prostatitis, there
is a salt (cup calcic) incrustation with sporadic or multiple infiltrates,
scars and closed suppurative cavities. An intense exfoliating of glandular and
transitional cellular elements is typical for chronic
nonspecific prostatitis along with the discharge of
inflammatory exudate.
In 89% of the patients the prostatitis is
accompanied by significant changes in seminal hillock and posterior urethra.
Systematic examination of the specified sections of urethral tract is of great
importance for diagnostics and treatment. Timely medical treatment of
urethritis and colliculitis is the primary prerequisite of successful treatment
and prevention of prostatitis.
The subjective and objective symptoms and
signs of prostatitis are notable for high variability and polymorphism. At the
same time, a common pattern can be observed in clinical presentations of the
prostatitis. To detect these presentations and to control the
patient’s conditions the
Chronic Prostatitis Symptom Index is used. It makes it possible to assess
pain and dysuric syndromes, as well as the quality of the patient’s living.
The subjective data, such as pain, sense of
discomfort in the region of anus, perineum, pelvic-lumbar region accompanied by
vegetal, copulative or generative disorders are typical for all forms of the
prostatitis. This picture is supplemented by particular signs.
General symptoms: rigor, temperature rise, general weakness, rapid fatigability,
sleep disturbance, excessive nervousness, and obsessions.
Local symptoms: prostatalgia, change in shape, size and consistency of the prostate
gland, high leukocyte reaction of the prostate gland secretion, extragenital
pain, pelvic sympathalgia, heaviness below waist, itching (urethra, perineum,
anus), paresthesias in genital organs (tickling feeling in the urethra,
creeping sensation, coldness of genital organs etc.), pathologic discharges
from urethra, more frequent desires to urinate, interrupted urine stream,
changes in seminal hillock, posterior urethra, changes in seminal vesicles,
rectum pathology.
Functional symptoms: intensification of spontaneous erections with underlying normal
adequate erections, intensification of adequate erections, weakening of
adequate erections, acceleration of ejaculation, inapparent orgasm, painful
orgasm, sexual frustration, no impregnation, changes in quantity of ejaculate,
pathospermia, primary sterility, secondary sterility.
Causative factors (infectious, hormone disruptions, immunologic, neurologic
alterations) are assessed individually. They are of great significance in the
patient treatment. When developing a treatment and prevention plan, any
contributory causes should be eliminated in the first instance.
Fife main tasks are settled in the
pathogenetic therapy which
should be conducted simultaneously with etiotropic one:
1) general and local
immunocorrection;
2) normalization of venal and arterial
components of blood supply to the prostate gland;
3) reconstitution of secretion outflow of
the prostate gland and seminal vesicles, Littre and Kuperovyh’s glands by means of muscles
hypertension of pelvis, perineum, smooth muscle fibres of the prostate
gland;
4) regeneration of structural and
morphological elements of pathologically modified tissues;
5) normalization of the complete range of
functions of the organs affected.
These tasks are successfully settled by a
complex therapy with the use of low-level laser irradiation.
Treatment of the patients suffering from
nonspecific inflammatory diseases of the prostate gland, seminal vesicles,
seminal hillock (prostatitis, vesiculitis, and colliculitis) should be
comprehensive and
ethiopathogetetic. However, many nonsurgical therapy techniques do not give the
desired effect. The situation is turning to better when the therapeutic complex
includes the exposure to ILBI of different spectral bands.
MLT mode, which includes a transrectoral
action, when the action is exerted directly on the prostate gland and
neurovascular bundle, exercising control of the organ’s function, in combination with
transcutaneous blood irradiation in the biocontrol mode that makes it possible
to make an immunocorrective action on the organism (BIO mode in Mustang 2000 or Mustang 2000+ laser therapeutic device), appeared to be the most
efficient.
Drug-free methods are often not only an
alternative for the conventional medicinal ones, but have also significant
advantages as methods of functional regulation. At the same time, an efficiency
of combination of various physiotherapy methods in combination with antibiotic
treatment is demonstrated. For instance, I.V. Karpukhin et al. (2000) recommend
to include in a multimodality therapy of prostatitis the LT, magnetic therapy
and phonophoresis of medicaments by means of low-frequency
ultrasound.
An interaction between the target organs and
testosterone metabolism organs is complicated and poorly known. It is proved
only that the liver is a source of hyperstrogenism, which causes the
significant reproductive and copulative dysfunctions. Chronic latently running
diseases of liver should be timely treated. Impairment of detoxification
function of liver results in testosterone metabolic misbalance. Therefore, an
action on the liver in the laser treatment mode takes one of the first
places.
Owing to the multicomponent and multilevel
action of ILBI, normalization of metabolism and blood circulation, a
multimodality therapy of urological diseases with the use of laser irradiation
is accompanied with improvement of the effectiveness of all therapeutic
interventions. Definite improvement of lymph and blood flows in the region of
laser exposure determines more effective entrance of antibiotic substances into
the prostate gland that makes it possible to reduce the quantity of the
required medicinal agents and the dosage of the medicines used.
The primary task of laser therapy is to
select the exposure parameters, technique and modality, which ensure the
maximum therapeutic effect in the absence of adverse effects. In case of
excessive increase of content of endogenic photosensitizers (in particular,
bilirubin) or overdosage of photo action, inhibition of phagocytic activity or
excess NO products is possible that may aggravate the run of the basic
disease.
Indications to laser therapy
application:
• chronic congestive prostatitis;
• chronic bacterial prostatitis;
• chronic prostatitis at urogenital infection after the second course of anti-infective therapy;
• copulative dysfunction;
• inter-receptive male sterility caused by prostatitis;
• neurovegetative prostatopathy;
• prostatitis with prostatic hypertrophy in the absence of prostate carcinoma;
• urethral stricture.
The laser therapy is an additional aid in
sub-acute and chronic periods of a disease contributing to sanitation of the
affected area and mobilizing the body defences. Achievement of high remedial
result, reduction of treatment period, improvement of drug bioavailability for
the prostate can be provided by observance of simple organizational and
therapeutic conditions. They include: reasonable diet, individual work-rest
rhythm, remedial gymnastics, compliance with the rules for sex life hygiene,
normalization of functions of the organs which participate in hormonopoiesis,
sedative medicaments if any psychoneurological symptoms, elimination of
potential infection pockets.
The laser therapy is conducted with
partially filled urinary bladder (for subsequent mechanical evacuation of the
prostate gland secretion with urine). The patient shall stay in an
urogynecological examination chair, lying flat on back that enables him to
relax maximally its skeletal muscles of the lower part of the body and lower
limbs. Action by laser radiation is intra-rectal (Fig. 17) and/or
transcutaneous on perineum (a region between marsupium and anus) through one
layer of gauze wipe (Fig. 18).

Fig. 17. Intra-rectal laser therapy of
prostatitis
Technique 1: intra-rectal, using Mustang 2000 or Mustang 2000+ laser therapeutic device. KLO3-2000 radiation probe, radiation
wavelength 0.63 µm, maximum output radiation power, within 1.5–2 minutes through a proctologic
attachment of P-2
type (Fig. 19) entered into rectum, on the prostate
gland projection (Fig. 17). It makes it possible to eliminate the inflammatory
processes in the gland, as well as to improve the blood flow in the tissues
within the exposure region. Such technique is recommended for use in the first
several sessions, especially in case of advanced form of chronic prostatitis,
as well as in the course of antibacterial therapy.

Fig. 18. Transcutaneous laser therapy of
prostatitis

Fig. 19. P-2 proctologic attachment
Technique 2: transcutaneous, using Mustang 2000 or Mustang 2000+ laser therapeutic device. Radiation of pulse infrared lasers,
wavelength 0.89 µm, pulse recurrence frequency 80 Hz, output radiation power
7–10 W for LO4-2000 radiation probe and
40–50 W for MLO1K-2000
matrix radiation probe, time of exposure
1.5–2 min. transcutaneously
(Fig. 18). Intra-rectal technique is also allowed for LO4-2000 radiation probe with
P-2 proctologic attachment
(see above).
Technique 3: BIO mode using Mustang 2000 or Mustang 2000+ laser therapeutic device. In this mode, phase coincidence of small
pelvis and perineum simulation (exposure techniques 1 and 2) with pulse wave
phase and 10 Hz modulation frequency is an additional factor improving the
functions of microcirculatory bloodstream which is the most affected by
pathological changes. Such mode is recommended for use in the final three
sessions of laser therapy for normalization of the prostate gland and central
(system) regulatory mechanisms functioning. Pulse recurrence frequency 3000 Hz
for pulse laser probes, time of exposure is increased to 5 min.
Technique 4: acupunctural, using Mustang 2000 or Mustang 2000+ laser therapeutic device. The possibility to conduct the
laserpuncture by means of continuous or modulated radiation of the red spectral
band (0.63 µm, radiation power at the A-3 acupunctural attachment output (Fig.
20) 1–2 mW) on acupunctural
points (AP) makes it possible to enhance the effects of the local laser action
and provides mobilization of sanogenesis system mechanisms, makes it possible
to rehabilitate the sexual function of the middle- and old age patients
[Belavin A.S., 1991; Veinberg Z.S. et al., 1979; Kulavskyi V.A., Kryukov L.A.,
1989].

Fig. 20. A-3 acupunctural
attachment
Laserpuncture on “basic prescription”
points is conducted immediately after the laser physiotherapy (exposure
techniques 1 and 2) in the following order [Builin V.A., 1997, 2002].
The laserpuncture shall be conducted by a
reflexologist.
On Monday,
Wednesday, and Friday – action on points GI-4 and E-36
symmetrically, then on point VC-12.
On Tuesday and
Thursday (Saturday) – action on points МС-6 and RP-6
symmetrically, then on point VC-12.
Exposition of corporeal AP is 10–20 sec. (not more than 30 sec). In case
of laser radiation modulation by frequencies 1...10 Hz restorative effect is
achieved mainly (exposure of one AP is 10 sec.), and by frequencies of 20...100
Hz – sedative (exposure
20–30 sec.). The optimum
frequency of the laser radiation modulation is 2.4 Hz (frequencies 1...5 Hz
– is a range of
physiological rhythm of the prostate gland functioning).
It is showed by the experiments that the
frequency of 1.2 Hz have a selective effect on cross-striated muscles of small
pelvis and perineum. The frequency of 5 Hz is optimum for action on the
smooth-muscle elements of the prostate gland, urinary bladder and straight
intestine. The frequency of 21 Hz promotes the improvement of the trophism of
nerve endings, restoration of their sensitiveness and
conductibility.
At the laserpuncture the reflexologist may
add to the “basic prescription” 2–3 points (depending on specific symptoms).
Prostatitis, vesiculitis, colliculitis:
V-40, VC-1, VG-1, F-8, F-3.
Asthenic neuroticisms, psychogenic sexual
dysfunctions: R-2, VG-4 (2.4 Hz
modulation).
Plan of the laser therapy of chronic
prostatitis without pronounced symptoms and gross structural and morphological
changes in the prostate gland. This plan can be
implemented for conduct of a preventive course of the prostatitis treatment.
There are used LO4-2000
radiation probe, radiation power 7–10 W, frequency 80 Hz, with ZM50 magnetic attachment (50 mT) and
MLO1K-2000 radiation probe,
pulse radiation power 40–60
W, frequency 80 Hz, with MM50 magnetic attachment (50 mT). The patient shall stay in seated or
prone position. Action on zones (Fig. 21) is made simultaneously by two
radiation probes in the following order:
• LO4-2000 radiation probe – zone 5 on one side of the body during
2 min., MLO1K-2000 radiation
probe – zone 4 during 2 min.;
• LO4-2000 radiation probe – zone 5 on another side of the body
during 2 min., MLO1K-2000
radiation probe – zone 1 during 2
min.
The patient lies on his side and moves his
kneels to the belly, MLO1K-2000 radiation probe is placed in the perineum (between anus and
marsupium root), exposure is provided through 1–2 layers of gauze wipe during 2 min.
Simultaneously, zone 2 is exposed to action of LO4-2000 radiation probe during 1 min.,
then zone 3 during 1 min. Upon completion of the session the patient shall rest
for 15-20 min. sitting.

Fig. 21. Exposure zones in laser therapy of
disease of male urogenital system organs
From the 4th session it is reasonable to add
laserpuncture of “basic prescription” points (2.4 Hz
modulation).
The course of laser therapy consists of 12
daily sessions (except for the weekend), it is reasonable to start the
treatment on Monday.
In treatment of advanced stages of the
prostatitis forms with pronounced symptoms and
objective changes in the gland the following plan of the laser therapy is
implemented.
Sessions 1–5. The patient is in examination chair;
KLO3-2000 radiation probe
(7–10 mW, 5 Hz modulation
frequency); straight intestine is exposed by means of P-2 proctologic attachment (a condom
shall be put on the attachment) during 4–5 min. Simultaneously, by MLO1K-2000 radiation probe (power
40–60 W, frequency 80 Hz)
with MM50 magnetic attachment one acts stationary on zones 4 and 1 (Fig. 21)
by contact with exposure time of 2 min. on each.
Upon completion of each session, the patient
makes breathing exercises staying in the examination chair. The
patient’s breathing pattern
during exercises is diaphragmatic; it means that the anterior abdominal wall
shall pulled out as he inhales, and pulled in as he exhales. The perineum and
pelvic floor muscles relaxation and tensioning controlled by the patient shall
coincide with the breathing patterns (as he inhales – tensioning, as he exhales – relaxation). During these exercises,
red ILBI (KLO3-2000
radiation probe, power 7–10
mW, modulation 5 Hz, А-3
acupunctural attachment) acts on acupuncture point VC-1 (perineum, the point is
located in the centre of the centre line connecting the marsupium root and
anus) during 2 min. Thereafter, the patient is recommended to relive himself,
and then to have rest during 15–20 minutes.
Sessions 6
to 9 inclusive: LO4-2000 radiation probes are used (7–10 W, 80 Hz, ZM50 magnetic
attachment) and MLO1K-2000
(40–50 W, 80 Hz,
MM50 magnetic attachment). The patient is in sitting position or lying.
Action on zones (Fig. 21) is made simultaneously with these two radiation
probes in the following order:
• LO4-2000 radiation probe – zone 5 on one side of the body during
2 min, MLO1K-2000 radiation
probe – zone 4 during 2
min.;
• LO4-2000 radiation probe – zone 5 on other side of the body
during 2 min, MLO1K-2000
radiation probe – zone 1
during 2 min.
The patient stands in the knee-elbow
position; MLO1K-2000
radiation probe is placed in the perineum (between the anus and marsupium
root), exposure is provided through 1–2 layers of gauze wipe during 2 min. Simultaneously, LO4-2000 radiation probe acts on zone 2
during 1 min., then on zone 3 during 1 min. After completion of the session the
patient shall have rest for 15–20 min. in the sitting position.
Sessions
10–12. Biosynchronized magneto-laser therapy is conducted. The heart rate
and respiration sensors are fixed on the patient (in the sitting position).
Timer on the device panel is set on 10 min. (laser action on different zones
shall be made continuously
during 10 min.). The radiation probes are moved within the zones without
switching off of ILBI so that the patient and doctor’s eyes were not exposed to the
radiation (the radiation probe is moved above the body surface at the distance
of 0.5-1 cm; exposure is controlled by the device timer like by stop watch).
Action on zones (Fig. 21) is made simultaneously by these two radiation probes
in the following order:
• LO4-2000 radiation probe (80 Hz,
7–10 W, ZM50 magnetic
attachment) – zone 5 on one
side of the body during 2 min,
MLO1K-2000 radiation probe (80 Hz, 40–50 W, MM50 magnetic
attachment) – zone 4 during
2 min;
• LO4-2000 radiation probe – zone 5 on other side of the body
during 2 min, MLO1K-2000
radiation probe – zone 1
during 2 min.
The patient lies on his side and moves his
knees to the belly (thereafter one should check if the heart rate and
respiration sensors are fixed securely). MLO1K-2000 radiation probe is placed in
the perineum (between anus and marsupium root), exposure is provided through
1–2 layers of gauze wipe
during 4-5 min. Simultaneously, one acts by LO4-2000 radiation probe on zone 2 during
2 min., then on zone 3 during 2 min. After completion of the session the
patient shall have rest for 15–20 min. in the sitting position.
Unsatisfactory or negative result of LT is
largely due wrong selection of dosages of laser and magneto-laser exposure,
disregard of psychosomatic condition of the patient and importance of
establishment of a good contact of doctor with patient.
If the conditions of the posterior
urethritis and colliculitis prevail, as well as the dysfunction of ejaculation
is pronounced, on conducts a transcutaneous, contact-mirror exposure
(LO4-2000 laser probe,
output radiation power 7–10
W, frequency 600 Hz) of the upper part of penis in its rear third and of its
root during 5 min. on a zone. If MLO1K-2000 pulse IR-laser probe is used – power - maximum, frequency 600 Hz,
exposure time also 5 min. for each zone. In addition KLO3-2000 laser probe of red spectrum
(0.63 µm) may be used with U-1 urethral attachment (Fig. 22) during 2 min.

Fig. 22. U-1 urethral attachment
V.I. Redkovich (1993) recommends to apply LT
more widely for the patients with chronic prostatitis complicated by sterility
due to high viscosity of ejaculate, reduction of mobility and activity of
erythrocytes because ILBI improves the copulative and reproductive functions of
such patients considerably.
The effect of laser and magnet-laser therapy
of the said forms of prostatitis and their complications is achieved already by
the end of the first course of treatment and confirmed by the
patient’s subjective value
and clinical laboratory studies.
13. Male Sexual Disorders
Erectile dysfunction (ED), a constant or
temporary inability to get or keep erection sufficient for making successful
coitus, is an important social and medical issue all over the
world.
Inability to get erection or keep it is the
most frequent failure which can trouble a man. The word ‘impotency’ took not only an offensive
connotation, but represents hardly anything of a complicated process of sexual
dysfunction presentations.
There are two kinds of male sex disorders:
reproductive failure and inability to perform
coitus.
The following ED classification is
recommended by the International Society of Impotence Research [Lizza E.F.,
Rosen R.C., 1999].
I. Psychogenic ED.
II. Organic ED:
1. Vasculogenic:
a) Arteriogenic;
b) Vein occlusive (cavernous);
c) Mixed.
2. Neurogenic.
3. Anatomic (structural).
4. Endocrine.
Dug induced ED, which is connected with
administration of various pharmacological agents, is distinguished as a
separate form of ED.
Until the early 1980s of the past century,
ED was considered largely as a psychogenic disease, but with the development of
diagnostic techniques organic causes of ED began to be detected in about 80% of
the patients [Melman A., 1995].
At present, the relationship between ED and
metabolic syndrome (MS), which is understood to be a combination of several
vascular risk factors, first of all, impaired glucose tolerance, abdominal
obesity, dyslipidaemia, and arterial hypertension (AH), attracts special
attention of the researches [Mazo E.B. et al., 2004, 2006].
It is noted that both, psychogenic forms of
disorders and pseudo-impotency in young men, and loss of status in the sphere
of importance in connection with the age-related reduction in sexual abilities,
change in usual type of sexual relations, result in formation of persistent
neurotic reactions with a decrease of interest in life. Currently, the most
common sexual disorders in men are erection
disorders, premature and retarded ejaculation.
There are two kinds of male sex disorders:
reproductive failure and inability to perform
coitus.
Sexual drive and sex satisfaction in men are
based on erection, ejaculation, orgasm and libido. Control of erection and
ejaculation as the complex reflex acts is performed at the level of VNS. While
being interrelated at normal sexual function, they can be subjected to painful
changes separately.
Male sexual potential is determined by
general psychophysical state which is maintained at the proper level by
sufficient physical activity and psychical equation technique. Strengthening
regularly the ligaments and joints and training major muscles involved in
sexual act, a man is able to increase their strength, endurance and flexibility
that ultimately will have a positive impact on the “end result”. Moreover,
any physical exercises activate the hormonal systems that result in increase of
epinephrine, endorphins and testosterone contents in blood without which
necessary amount the normal erection is impossible in general.
It is known that in case of regular sexual
relations, the hormones such as epinephrine and cortisone, which stipulate the
blood circulation, cerebration and prevent blind headaches, provides an
opportunity to maintain an excellent psychophysical status, are generated in
the organism. A love intercourse burns about 150 calories, i.e. it substitutes
30-minute jogging. Moreover, the heart rate quickens up to 160 beats per minute
for a short time, and blood pressure is doubled for a while that is extremely
useful for training of the heart-vascular system. The content of oxytocin, a
hormone which relieves depression and loneliness, increases by 3.5 times in the
climaxed organism. Other hormone, epinephrine, suppresses pain like morphine
but without destroying consequences for the organism. One more hormone,
cortisol (hydrocortisone) is required for people suffering from arthritis.
According to the American scientists, the capacity to work falls down
drastically in 70% of women and 25% of men if they experience sexual problems.
The same cause gives rise to 60 to 100% neurosis.
The genital sphere of any human as an
important element of maintenance of physiologic equilibration is included in
the net of endocrine and vegetative systems that provides fine regulation of
all systems and organs; moreover, these links are double-way. As it well-known,
the small pelvic organs have strongly developed vegetative (sympathetic and
parasympathetic) innervation.
The following diseases are attributed to the
psychosomatic diseases of genital sphere:
• impotency;
• premature ejaculation;
• male sterility.
Any stress and emotional tension reduce
considerably the organism resistance (in this context, any disease may be
considered to be psychologically associated). If a failure in the work of brain
cortical divisions, VNS or endocrine system occurs caused by frequent and
long-term psychoemotional over-tensions, infections, intoxications, traumas
etc. (diagnosed to be neurosis, vegetative dystonia, hyper- or hypothyrosis
etc.), it results in dyscrasia (flowing equilibrium of internal environment)
and development of various syndromes of the secondary affection of organs,
tissues. There is also a feedback: pathogenetic role of somatic pathology in
the development of neuropsychic disorders.
Large number of patients suffer from
psychogenic impotency with pathologic over-excitation of ejaculation function
and pathologic inhibition of erection function. The impotency forms with
over-excitation are developed more frequently in the patients with neurasthenic
and hysteric neurosis, with inhibition – in patients with obsessive-compulsive neurosis.
The impotency sends signals on the following
troubles:
• neurotic disorders, depressions (in 75–90% of the cases);
• pancreatic diabetes;
• alcohol dependence, narcomania, organism intoxication;
• metabolic disturbance (up to 10%).
In the event of these diseases, blood supply
to various organs, pulse transmission via sensigerous and motor fibres are
disturbed, which means that the reflex arc that ensures the erection suffers,
too. The problems with sexual potency occur sometimes after traumas or diseases
of spinal cord and brain. Often, disturbed erection is the first symptom of an
infectious affection, trauma, tumour, epilepsy or Parkinson’s disease. The impotency can be
developed as a bad effect of drug administration. Any counter-depressants,
neuroleptic agents, antianxiety agents, agents for hypertension treatment, and
agents, which reduce the gastric secretion, have an impact on erection.
Analgin, antihypertensive drugs, smoking and alcohol reduce sexual drive;
suppress erection and retard ejaculation. The content of testosterone in blood
decreases with age in certain diseases.
There is a term in the world sexual medicine
“businessman syndrome”, which means decrease of sexual activity in the
absence of any diseases. This syndrome means the development of stagnations in
the small pelvis due to improper sedentary lifestyle and high psychological
stresses, excessive smoking, misbalanced nutrition. Due to smoking, in 8 cases
out of 10, vasoconstriction occurs in male genitals, and as a result
– impotency. The smokers
have 2 times more chances to become a sexual impotent than the non-smokers (up
to 50% of the examined smokers suffer from sexual impotency to a greater or
lesser degree). In accordance with the results of a research, it was noted the
absence of sex drive (libido) in more than 56% and reduction of sexual potency
– in 46% in a group of men
having being involved in business for 5–8 years.
The maximum time limit for a male drinker is
15 years. If he took his first glass of port wine when he was 15-16 years old,
he has very seriously to give thought to the fact how long he will remain a
“man”. The man does not want to admit to himself that the reduced sexual
potency is caused by allocation of alcohol and…he goes to an urologist. The
latter, having found nothing special and having not analysed the situation well
and being afraid to admit it, makes a diagnosis of “chronic prostatitis”.
The patient is being treated, but his sexual function is never normalized. The
drinkers find fault mainly with detumesco (sudden disappearance of erection
during the sexual congress). The treatment is possible provided of
unconditional refusal of alcohol for a long term.
Deficiency of testosterone is found in every
fifth man with age. As a rule, the symptoms of testosterone deficiency are not
given enough attention resulting in serious problems with health, including
osteoporosis and depression. An early diagnostics is required first and
foremost. As a general rule, special attention should be paid to the elderly
men with the symptoms of hypodynamia, problems with erection, loss of energy
and interest in sex (libido), depression and mood swings, problems with
attention concentration, decrease of muscle bulk and hair covering on breast
and troubled sleep.
It is important to exclude causes such as
pituitary tumour and damage to the testicles. Decreased testosterone level in
boys and adolescents may have a genetic condition. Along with the blood tests,
the level of other hormones, the condition of the pituitary gland and bones are
diagnosed, the analysis of seminal fluid is made and the prostate gland is
examined.
Sexual dysfunction in man includes disturbances of libido (sex drive), penile erection
(erectile dysfunction, ED) and ejaculation (emission of seminal fluid), but not
necessarily all they are observed in one patient. In particular, those erectile
dysfunctions occur most often, for which treatment the most intensive and
effective arsenal of medical and surgical aids is proposed. It should be noted
that the above list of sexual function disorders is called sometimes sexual
dysfunction. However, in endocrinologic practice the term of sexual dysfunction
includes a wider range of issues, in particular, disturbance of genital glands
hormone regulations, their influence on the processes of puberty, metabolic
processes, and others. Therefore, it is reasonably to define the disturbance of
sexual relations as sexual dysfunction considering it as one of the aspects of manifestation of endocrine
sexual dysfunction if it occurred, for example, in connection with
hypogenitalism.
Among the men with diabetes, ED occurs in
50-70% of the cases, and occurs at a younger age (within the first 10 years of
illness) than in the population as a whole. Among people with diabetes aged
20-29 years it occurs in 9% and increases to 95% at age of 70. It is noted that
the ED may be the first sign of diabetes of the second type. ED may be an
indirect sign of generalization of atherosclerotic vascular disease in diabetes
and coronary heart disease progression harbinger.
Acetylcholine and some non-adrenergic,
non-cholinergic messengers are neurotransmitters of nerve endings involved in
the erectile response. The end neurotransmitter is an active vasodilator -
nitric oxide (NO). The latter increases the level of cyclic guanosine
monophosphate (cGMP) in smooth muscle cells of the penis which activates
relaxation of smooth muscles of erectile tissues. This ultimately causes the
erection, cGMP further is split in the erectile tissues under action of
specific for cavernous body phosphodiesterase of the 5th type and detumesco (return to its
original state after erection) occurs.
Peripheral nerves have sensory and motor
elements, which constitute a part of the reflex arc closed in spinal cord in
the region known as spinal erectile centre. Consequently, so-called "reflex"
erection can be caused by direct stimulating effect on penis is not only in
healthy people, but also in the patients with spinal cord suprasacral
intersection.
At the present time, one can call main
pathogenesis links of neurosomatic affections. Firstly, it is neurotrophic and
neurovascular disorders. Secondly, an excessive or inadequate production of a
hormone. All this results in significant alterations of homeostasis (disorders
of protein, carbohydrate, fat, water electrolyte metabolism, acid-base balance,
etc.) and disorders in metabolic processes in cells and tissues. The prominent
Soviet pathophysiologist A.D. Speranski came to the conclusion that a
nonspecific neurotrophic component is necessarily included in the pathogenesis
of any disease process (infectious, traumatic, psychosomatic etc.). This was
further confirmed by many experiments and clinical data.
Pathologic pulses reach a particular organ
or several organs mainly via sympathetic nerves that results, in case of
prolonged exposure, in depletion of tissue reserves of norepinephrine and
development of local or diffuse dystrophies. The experimental studies are
consistent with clinical observations which showed how neuroses and vegetative
functional disorders can eventually culminate with an organic disease -
resistant arterial hypertension, stomach ulcers, gangrene of limbs, myocardial
dystrophy, etc. Any organ and tissue dystrophies are based on its reflex
nature, i.e. unusual in strength and duration of stimulation. Sympathetic
nerves are an effector way by reflexes disturbing trophism, and the immediate
cause - the release of noradrenaline at the ends of the nerves in a very high
concentration. Another pathogenic factor is a disorder of homeostasis (often
relatively selective: in the heart, lungs, liver, muscles, skin, etc.) due to
insufficient or excessive generation of hormones and mediators (ACTH, growth
hormone, mineral and glucocorticoids, thyroxin, adrenaline etc.) [Krupin V.N.,
Serova S.V., 1992; Martynov Yu.S. et al., 1980].
The data accumulated at present indicate
that the central link of pathogenesis of any neurosomatic disturbances is
hypothalamic-pituitary. In case of an excessive nervous tension and conflicts
the regulating effect of the brain on the lower levels of vegetative nervous
system and the endocrine glands is disarranged. In some cases, the pathogenesis
of the disease is caused by a relatively selective involvement of VNS, in other
cases - by endocrine glands. A type of emotions (fear, anger, doubt, joy, etc.)
has certain importance for the nature of psychosomatic diseases development; it
determines a specificity of excitation of the regulatory systems, the acuteness
of the process. Reflexologists know the connection of each kind of emotions
with a specific organ (e.g., anger is connected with liver, it damages it).
Unpleasant thoughts, heavy thoughts, doubts, remorse result in neurotrophic and
neurovascular disorders and diseases.
The feedback is also proved: a pathogenetic
role of somatic pathology in the development of neuropsychic disorders. A
pathological pulsation with development of repercussive and generalized reflex
syndromes (vegetovascular dystonia, neurasthenia, reflex paralysis,
contracture, and hyperkinesis) can occur from an affected organ. Radicular and
neurasthenic syndromes and vegetative endocrine disorders are often observed in
the patients suffering from chronic inflammation of the prostate. General
symptoms of prostatitis are nonspecific: it is general weakness, sleep and mood
disturbances, fatigability, performance impairment, well-being variations
during the day. But main symptom is a painful and difficult urination. The
sexual dysfunctions are often the only complaint of the patient with
prostatitis. Hormonal imbalance results in decrease of sexual desire, rare
sexual congresses and, consequently, to stagnation in the prostate gland, which
closes the "vicious circle" of the disease. Another complaint of the people
suffering from prostatitis is sterility.
Treatment of functional and organic diseases
of genital organs, as well as sexual dysfunction is a topical and complicated
problem. Currently, there are used practically all kinds of local and systemic
treatments of this pathology known in medicine. In case of neurogenic form of
impotency, it is quite effective the use of a variety of physical factors, in
particular, the magnetic field [Myasnikov I.G., Krupin V.I., 1992],
galvanization, medicine electrophoresis, an electric field UHF, decimetre waves
and sinusoidal modulated currents, mud, naftalan and clay applications
[Karpukhin I.V., 1991; Karpukhin I.V. et al., 1991], acupuncture [Jingzhong W.,
1989; Muccioli M., 1990]. The effectiveness of physiotherapy increases greatly
against the medical treatment conducted concurrently. If there are any signs of
failure of the sympathetic-adrenal system (adynamia, apathy, drowsiness,
hypoglycaemia, and hypotension), then the inclusion of stimulants, including
hormones, in the scope of therapeutic agents, can have a beneficial effect on
the disease. On the contrary, if an excessive over-excitation of the system
(insomnia, increased blood pressure, tachycardia, hyperglycaemia,
hyperadrenia), it is the prescription of the agents of ganglioblocking and
neuroleptic action that usually improves the condition of the patients and can
prevent the development of dangerous complications associated with the
depletion of catecholamines and acetylcholine in the nervous system and various
organs and tissues
Organic causes of
sexual dysfunctions need another approach and another treatment method. About
25% of the men, having had traumatic brain injury, suffer from sexual
dysfunctions, 99% of the men with diseases and spinal injuries have affected
erection function. Any hurts and injuries of penis make the sexual congress
difficult or impossible at all. In 70% of the men the decrease of male
fertility is caused by an infectious disease. Even the diseases such as
influenza, pneumonia, otitis, can cause loss of erection in any man.
It should be noted that up to 30% of the men
among the patients with erectile dysfunctions (ED) suffer from pancreatic
diabetes and 40% - from vascular abnormalities (in total 70%), and diabetes is
main cause of vascular affections. Other factors of ED are relatively rare,
they include: hypothyroidism, hypogenitalism, adipose, smoking, disseminated
sclerosis, chronic renal insufficiency, surgical or traumatic injuries of
penis, prostate gland, urinary bladder, pelvis and spinal cord structures,
alcohol impact, medications for treatment of arterial hypertension,
antihistaminic medications, antidepressants, tranquilizers, anorectic agents
and Cytimidine. The male fertility is reduced due to full and even partial
starvation.
The treatment of the patients with sexual
disorders should be complex subject to a close professional collaboration of
doctors of different specialties: urologist, therapist, neurologist,
psychotherapist, and sexologist. Modern operative and orthopaedic equipment is
extremely effective in case of organic pathology of the sexual
sphere.
The laser treatment of sexual disorders has
significantly expended the therapeutic possibilities of modern sexologists and
reflexologists. It is due to the fact that LLLT is sufficiently effective in
case of organic sexual disorders caused by somatic pathology, and in case of
secondary affections due to traumas or disease. Thanks to the systematic
exposure to laser radiation, to the effect of “energy swap” the
normalization of functioning of almost all systems of the organism
occurs.
The control of erection and ejaculation as
complex reflex acts occurs at the level of vegetative nervous system;
therefore, their repair can be successfully resolved by methods of
reflexotherapy [Ivanov V.I., 1991; Fomberstein K.B., 1991]. It is demonstrated
high efficiency of combined and associated LT of various diseases of urogenital
sphere and sexual disorders [Vozianov A.F. et al., 1990; Kovalenko V.V.,
Kovtunyak O.N., 1990; Kushniruk Yu.I. et al., 1988; Reznikov L.Ya. et al.,
1988]. The modern techniques of combined exposure to optical (laser) and
microwave (EHF) bands are promising [Brekhov E.I. et al., 2007].
Numerous studies and clinical practices have
definitely proved the high efficiency of laser reflexotherapy in case of
various pathology, including in the sexual sphere [Beleda R.V., Taktarov V.G.,
2002; Builin V.A., 1998; Yasinki B.V., Zhyboryev B.N., 1988]. The laser
stimulation of acupuncture zones enhances the immune resistance potential,
nonspecific resistance of the organism, normalizes the regional and systemic
neuroendocrinal and microvascular control. The laser reflexotherapy with the
use of “basic prescription” of acupuncture points and combination of
specific corporeal and auricular points, as well as local negative pressure
(LNP) [Beleda R.V., Taktarov V.G., 2002; Kovalenko V.V., Kovtunyak O.N., 1990],
makes is possible to eliminate or significantly reduce any neurasthenic,
psychasthenic and depressive components of sexual disorders . A complex of
yearly rehabilitation based on LNP technique with simultaneous exposure to red
diodes improves the penile circulatory dynamics, increases oxygen saturation,
mitigates the risk of local fibrosis of albugineous tunic preventing any
secondary damage of venoocclusive mechanism occurring after remedial surgical
procedures on penis venous basins of the patients with vasculogenic form
of erectile dysfunctions [Yerkovich A.A., 2007].
Indications to
apply LT [Laser Therapy of Sexual Disorders, 1997]:
• various clinical variants of damages of vascular component of
copulatory interval erection component;
• psychogenic form of disorder of psychic component, particularly, in
case of misfortune expectation neurosis;
• debut form of impotency;
• rapid ejaculation;
• chronic prostatitis and prostatevesiculitis, especially with
underlying congestion in small pelvis;
• absistent forms of dispontecy;
• as
an element of sexual rehabilitation complex of the patients after
edenomectomy;
• Peyronie’s
disease;
• copulative dysfunction in the patients operated for urethral
stricture;
• potency disturbance after cavernitis;
• as
a final (rehabilitation) stage after penis vascularization;
• as
a final treatment stage of phalloplasty operation and in case of epi- and
hypospadias, micropenis;
• intermittent priapism.
Contraindications to apply LT:
General:
• any tumours (including prostate adenoma);
• hypertensive disease in stage III;
• pronounced arterial sclerosis of heart and brain;
• serious chronic disease of internals (glumeronephritis,
pancreatitis, hepatitis etc.) in the exacerbation phase;
• serologic disorders caused by endogenetic processes.
Local:
• inguinal and inguinoscrotal hernias;
• pampinocele of the 2nd and 3rd
degree;
• thrombophlebitis of pelvis and lower limb venaes;
• hydrocele and funicle membrane hydrocele;
• phimosis and paraphimosis;
• acute and chronic diseases of testicle and epididymis; acute
inflammatory disease of genital organs;
• photodermatotis.
In case of any sexual disorders accompanied by inflammatory and degenerative
processes in the prostate gland, the treatment begins
with a local action on the affected areas (see section “Prostatitis”).
After a 2-3 week break the laser reflexotherapy is carried out in accordance
with the plans below. The parameters of laser stimulation of acupuncture points
are referred to in section “Prostatitis”.
Composing a prescription, one adheres to the
principles of Zhen-Chiu therapy. [Laser Therapy of Sexual Disorders, 1997]. A
set of PA of general effect is distributed by weekdays in accordance with the
canons of the modern acupuncture and recommendations of the modern
chronomedicine. 4-6 points are used during one session. Ratio of corporeal and
auricular PA is 2:1. One tries to select PA of general and local actions in
approximate the same ratio. The laserpuncture sessions are carried out daily
within the first half of day (it is well know that maximum generation of
testosterone and minimum of antisexual hormone occurs in the man in the
morning) during 10-12 days. If necessary, the course is repeated in a
2–3 week break. The basic
prescription is supplemented with points GI-11, С-7, TR-5; among the
local and segmental corporeal points the points V-23, V-31, V-32, V-33, V-34,
F-5, Е-11, VC-2, VC-3 and VC-6 are the most frequently used. Auriculotherapy
is carried out on АР-13 –
adrenal gland point, АР-22 – glands of internal secretion point, АР-32 – testicle point, АР-56 – pelvis point and АР-58 – sexual point, АР-95 – kidney point, АР-79 – point of external sex
organs.
In case of erectile insufficiency with normal ejaculation and retained
libido the following plan of the laser reflexotherapy
can be recommended:
1st day: Е-36, RP-6;
2nd day: МС-6, VG-2, АР-58;
3rd day: С-7, VG-3, VG-4, АР-58, АР-79;
4th day: TR-5, V-31, V-32, АР-56, АР-95;
5th day: Е-36, V-31, V-32, V-33, АР-95;
6th day: GI-4, VG-3, VG-5, АР-22, АР-32;
7th day: С-7, V-27, V-28, V-29, АР-22;
8th day: TR-5, V-27, V-28, АР-32;
9th day: МС-6, VC-2, VC-6, АР-79;
10th day: GI-4, R-11, VC-4, АР-13;
11th day: RP-3, RP-4, VC-3, АР-58;
12th day: Е-36, GI-11.
Action on symmetrical points is made on both
sides of the body.
In case of normal
erection and rapid ejaculation action on PA of
“basic prescription” by low-frequency modulation (up to 20 Hz) is used.
Additional action is provided on several local and segmental AP points: VG-3,
V-28, V-25, V-31, V-32, V-33, V-34, R-10, R-13 и R-11. Among the points on
concha of auricle the most indicated for treatment are АР-22, АР-55,
АР-58, АР-79 и АР-93.
Approximate plan of AP selection for the
laser reflexotherapy:
1st day: RP-6, Е-36;
2nd day: F-5, VC-2, АР-55;
3rd day: Р-6, VC-2, VG-4, АР-58, АР-79;
4th day: GI-4, V-31, V-32, АР-58, АР-32;
5th day: RP-6, V-31, V-33, АР-22;
6th day: С-7, VG-4, VC-3, АР-55;
7th day: GI-4, VC-4, VC-5, АР-32;
8th day: F-6, RP-8, VC-7, АР-93;
9th day: F-5, Р-11;
10th day: RP-6, Е-36.
In case of misfortune expectation neurosis, erection disorders with underlying psychasthenia or depression of various degree of
manifestation it is necessary to add the points R-7, R-3, R-10 and F-1.
Auriculotherapy on points АР-22, АР-79, АР-95 и АР-97. Action is made
in accordance with the plan:
1st day: Е-36, GI-4, GI-11, VC-12;
2nd day: GI-4, RP-6, АР-55, VC-12;
3rd day: МС-6, V-23, АР-34;
4th day: С-7, V-25, VG-4, АР-93;
5th day: F-2, F-4, АР-22, АР-95;
6th day: Е-36, Е-30, VG-3, АР-97, АР-58, VC-12;
7th day: RР-9, R-12, VC-4, АР-23, АР-25;
8th day: VC-2, VC-3, VC-6, AP-113;
9th day: GI-11, Р-10, VB-31, АР-34;
10th day: Е-36, МС-6, АР-58, VC-12.
For treatment of the patients with
spermatogenesis abnormalities, especially with underlying neurohumoral alterations present, the
corporeal points are used: VG-4, VG-3, V-23, VC-1, VB-20, С-7, VC-6, МС-7.
Laserpuncture of these points results in a remarkable increase of luteinizing
hormone of blood plasma and testosterone, and thus, particularly indicated if
there is a need to increase the sperm motility in case of asthenozoospermia. In
this case АР-16, АР-17, АР-32 и АР-22 are used.
An important issue is the compatibility of reflexotherapy with
basic drugs and physiotherapeutic procedures. The practice shows that in
laserpuncture the vitamins, antibiotics, analgesics, adaptogens and
immunomodulators may be used. It is unacceptable to take simultaneously any
drug changing the vegetative tonus, vasoactive and psychotropic agents. After
receiving antipsychotics, tranquilizers, antidepressants, steroids,
vegetotropic medications at least 3 weeks should pass before you can start the
laser reflexotherapy. According to the canons of classical Zhen-Chiu therapy,
other physiotherapeutic treatments should not be carried out also. However,
based on the clinical experience, we can recommend the simultaneous massage of
the prostate and seminal vesicles, baromassage of segmental points on back and
waist, exposure to local negative pressure (LNP) on the penis or carrying out
of a dosed local hyperthermia of the prostate gland. Point massage in case of
weakening of erection and ejaculation is made by stimulating method alternating
with relieving massage, and in case of premature ejaculation (but normal
erection) relieving method is used only [Tsutsumi I., 1984].
Upon completion of the first course of laser
therapy a 3-week break should be done. Further treatment (the 2nd and 3rd courses, and then, in a 6-month break,
the protracted treatment is repeated if necessary) is aimed at normalization of
disturbed functions of various systems taking into account the specific
symptoms and signs of each patient. Mainly, it is laser reflexotherapy, which
can be combined with other methods of reflexotherapy (microneedles, application
by medicinal substances, metals, hammer bone, acupressure etc.), but if the
treatment of a related somatic pathology is required, laser physiotherapy is
applied also in accordance with special techniques.
After 2–3 courses of physical- and
reflexotherapy it is reasonable to carry out a course of the systemic
energoinformational therapy – colour therapy. The method has been known for several millenniums
and is used traditionally in India, China and other oriental countries. There
are used light-emitting diode radiation probes of red SO3-2000, yellow SO4-2000, green SO5-2000 and blue SO6-2000 colours (Fig. 13) for
Mustang 2000 or Mustang 2000+ device. The colour therapy is carried out in 2 weeks after
completion of a laser therapy course. Action is made on exposed body areas, the
surrounding areas are covered with clothes. After connection of the relevant
light-emitting diode radiation probe to Mustang
2000 or Mustang
2000+ device, the radiation
power is increased to the maximum value. The radiation probe is located at the
distance of 1 cm far from the skin surface. Point zones are treated stationary.
To treat large areas the light-emitting diode radiation probes of matrix type
of red MSO3M-2000, yellow
MSO4M-2000, green
MSO5M-2000 and blue
MSO6M-2000 colours (Fig. 23)
are used.

Fig. 23. Appearance of light-emitting diode
radiation probes of matrix type
I. View of display panel. II. View of window
for radiation outlet.
The plan of colour
therapy course is as follows:
1st session: action on perinea region with
blue colour within 15 min. (a zone before anus), on omphalus – with green colour within 1
min.
2nd session: blue colour on perinea region
– 20 min., green colour on
omphalus within 2 min.
3rd and 4th
sessions: yellow colour on heels (within 5 min. on
each), on the point above symphysis (along median line) – 5 min., on sacral region and perineum
before anus – within 10
min. each.
5–8th
sessions: green colour on heels – 5 min. each, above pubis – 5 min, on perineum and sacral region
–10 min. each, on omphalus
– 1 min.
9–12th
sessions: red colour on the region from LV to SIV
– 15 min., yellow on the
region of ThX–LI
– 10 min., blue on vertex
– 10 min.
The colour therapy under this plan
contributes to effective treatment of prostatitis, stimulates the endocrine
glands and potency, renal function, and recovers from depression.
The laser- and colour therapy can be
repeated in 6 months if necessary.
14. Laser-vacuum therapy technique
The method of treatment of the patients with
erectile dysfunction combining action with negative pressure and phototherapy
is well-known [Builin V.A., 1998; Builin V.A. et al., 2004; Zelyenchuk A.V. et
al., 2003; Laser Therapy of Sexual Disorders, 1997; Loran O.B. et al., 1998;
Okovitov V.V., 2007; Shaplygin L.V. et al., 2004]. However, until recently, in
all commercially available devices and complexes action by light-emitting diodes was used, i.e.
there was applied the method of vacuum
phototherapy. At the present time, a complex for
laser-vacuum therapy of the patients with erectile dysfunction, the so-called
method of local laser negative pressure (LLNP) or laser vacuum therapy (LVT) is
applied in Russia.
V.I. Yakushev et al. (1989) included LLLT
and the method of non-invasive blood irradiation, consisting of transcutaneous
action on venous blood circulating in the cavernous bodies in large volumes in
the course of the session of erectile disorder treatment by method of local
negative pressure (LNP) for the patients suffering from disturbance of
copulative function. For this purpose, the process vessel of the unit for LNP
therapy was equipped with a laser source and a tank for immersion medium. O.K.
Yatsenko (1996) showed in his study the efficiency of the companied action of
ILBI and LNP.
Before to conduct the first session, any
patient should:
• fill in the form “International Index of Erectile Function”;
• understand the meaning and technique in an intelligible
form;
Special attention of the patient should be attracted to the
available pressure regulating buttons and switch buttons on Mustang-VACUUM-DynaVac vacuum massage device (Fig. 24), having explained to him that he can reduce the vacuum intensity in the vacuum cup (or switch off the device at all) at any time (in case of discomfort).

Fig. 24. Mustang-VACUUM-DynaVac vacuum massage
device
The patient is positioned on a couch or
(better) seated on a chair. His penis is placed into the vacuum cup, the
marsupium remains outside. The marsupium skin is pulled back and held by the
patient’s hand so the first
few minutes after the start of the session. It is important to achieve the best
fit of the vacuum cup by applying sterile gel on its adjacent end. Also, it is
recommended to apply the gel on the dorsal surface of the internal part of the
cup, on which the urethral surface of the penis rests to prevent any injury of
the cavernous bodies (due to torsion) and frenulum (friction against the
internal surface of the vacuum cup) at the start of negative pressure. In some
cases the patient is recommended to remove preliminary the hair within the area
of use of the device.
The vacuum cup is connected to Mustang-VACUUM-DynaVac vacuum massage
device by means of a connecting tube to create vacuum. The doctor sets the
required parameters of the treatment procedure using the controls on the front
panel and switches on the device. The value of negative pressure is set
individually for each patient. The required parameters of laser-vacuum therapy
are determined by trials. The practice shows that the initial weak erection
occurs if the pressure is reduced to 15-20 kPa.
The first session should be started with
pressure of 20 kPa, increase or reduce it gradually depending on the sensations
of the patient. By completion of the first session, the negative pressure
should be brought to not less than 25 kPa againt the habituation.
The combined LSO-TED laser-and-light emitting diode
radiation probe (Fig. 25) is connected to two channels of Mustang 2000 or Mustang 2000+ device. This probe is completed with 8 IR-laser diodes of purse
radiation mode with wavelength 0.89 µm of 60 W total maximum power, and with
18 red diodes of continuous mode with wavelength of 0.63 µm of 75 mW total
maximum power. The laser diodes are located on the probe in such a way that
provides the maximum efficient impact on the cavernous bodies. One connection
cord of the probe connects IR-laser pulse diodes (channel 1), the other one
– red diodes (channel
2).
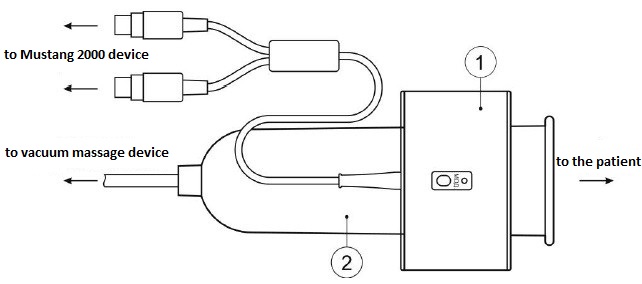
Fig. 25. LSO-TED combined radiation probe (1)
on vacuum cup (2)
In the course of the session the doctor and
patient observe the status of penis through the transparent walls of the cup.
Local reduction of atmospheric pressure in the vacuum cup wherein the penis is
placed causes an intense affluxion of blood to the cavernous bodies causing
passive erection of penis.
The treatment sessions are conducted under
the visual supervision control and a verbal contact with the patient within the
range of maximum reduction of pressure to 35–40 kPa. Even in the absence of
unpleasant sensations in the region of balanus it is not reasonable to reduce
the pressure by more than 40 kPa. The vacuum is maintained within up to 60
seconds at the required level of pressure release by 30–35–40 kPa, thereafter the pressure is
smoothly increased within 10-15 seconds to initial one.
In case of the need of rapid (emergency)
increase of pressure, when the patient feels pain in his penis balanus, the
button of compressor shutdown should be pressed immediately. In the normal
state of the patient’s
health the vacuum exposure is repeated in 10-15 seconds of break. Nr. 12-15
cycles (“ups” and “downs”) are performed during one treatment session.
The treatment course includes, on average, 12-15 (up to 20) sessions of
laser-vacuum therapy. The first 8–10 sessions are conducted daily, the rest – with break of 1-2 days (on average, 3
times per week).
The laser radiation shall be performed as
follows: if the companied LSO-TED radiation probe is used, switch on Mustang 2000 or Mustang 2000+ basic unit in sequence first the channel with red light-emitting
diode radiation at the carrier frequency in biomodulated mode in accordance
with the heart and respiration rates, and then the channel with the connected
IR-laser pulse radiation. The above actions by each of the channels should be
made during all cycles of pressure variation. The recommended total time of one
session – 12 min. (by 6
min. for each type of radiation). During a session of laser-vacuum therapy the
number of cycles and their duration should not be brought till occurrence of
oedema of penis prepuce.
Criteria of positive dynamic of
laser-vacuum therapy:
• pronounced lasting erection of penis already in the first cycles of
changing pressure in the cup;
• spontaneous morning erections become more frequent;
• improvement of libido;
• rehabilitation of ability to conduct a sexual
intercourse;
• rehabilitation of quality of erections in a sexual
intercourse;
• >increase in the duration of sexual intercourse.
Unacceptable errors when conducting the
laser-vacuum therapy
Own clinical experience and communications
with the doctors working under this techniques enabled me to reveal the most
frequent and typical errors in the session technique.
1. Failure to observe the depressurizing mode. If depressurizing in the vacuum cup is conducted too quickly (in
properly conducted session the depressurizing to 40 kPa should be achieved
within 20–25 seconds),
while not all cavernous bodies of penis are extended and filled with blood,
then pubis skin and subjacent cellular tissue is sucked into the cup causing
disturbance of blood flow and preventing erection.
2. Excess level of depressurizing in vacuum
cup up to 50–60 kPa and
more, “till it withstands”. In this case,
overstretching of cavernous tissues and blood vessels occurs; it can result in
rupture of a cavernous body with subsequent possible development of cavernous
fibrosis.
3. Exposure at the value of pressure
reduction of 40 kPa not within 40–60 seconds but 5–6 minutes and more. It is particularly
gross error sharply disturbing blood circulation in the penis causing multiple
haemorrhages with the subsequent degeneration and atrophy of cavernous
bodies.
4. Unjustified increase in the number of
sessions. Prescription of more than 15–20 sessions per one course of treatment
is not reasonable and results in undesirable results. A distinct effect appears
already after 4th
– 5th session provided that the sessions are
conducted properly.
5. No sufficient contact with the patient
in the course of session. Underestimating of the
patient’s sensations, his
complaints can result in a variety of unpleasant consequences, ranging from
oedema of prepuce with development of temporary phimosis to the development of
syncopal state.
Contraindications to laser-vacuum therapy
are:
• acute inflammatory diseases of prostate gland and urethra;
• urogenital zone skin diseases;
• sickle-cell disease;
• neoplasms of penis;
• mental illnesses;
• necessity to use antiaggregants regularly;
• Peyronie’s disease;
• trauma and operative interventions in the penis in the past medical history.
15. Traumatic ureteric fistulas
The secondary stenosis occurs often at the
place of ureter implantation after plastic surgery on the lower third of
ureter: inflammation in the zone of anastomosis and surrounding tissues
resulting in long-term anastomostitis due to claviform oedema and
post-operation trauma. Often, so-called irritable bladder is
formed.
Laser therapy shall begin from the first day after operation and is conducted
daily using Mustang 2000 or
Mustang 2000+ laser therapeutic device. LO4-2000 radiation probe, pulsed power
7–10 W, frequency 80 Hz.
Contact-mirror technique. Action on zones 3, 4 and 5 (Fig. 9) within 2 min. per
each zone.
16. Urogenital infection, urethritis
Increase in sexually transmitted diseases
makes to search the new approaches to solve this problem. According to the
literature, main group among the agents of disease are chlamydia,
mycoplasmosis, ureaplasmosis and gardnerellosis. For instance, more than 50
million people in the world are affected by urogenital chlamydia, and its
occurrence is 2-5 times more than gonorrhoea. Such high rate of infection
contamination of the population makes it necessary to develop the new, more
efficient tools and methods of diagnostics, treatment and rehabilitation of the
patients with this pathology.
The relative share of urethritis, cervicitis
achieves 60–70%. Often,
chlamydia is combined with ureamycoplasmosis and has weak clinical
presentations and it complicates the timely treatment. Chronic forms of the
disease often resulting in sterility dominate as a result of infection with the
mixed urogenital flora.
Treatment of chronic infectious urethritis
is currently a major challenge. The literature provides plenty of therapeutic
treatment schemes, but the most efficient appeared to be a complex approach
proposed by S.N. Dzhumaliyev et al. (2000), who applied in chlamydial and
ueramycoplasmal infection a specific antibacterial therapy taking into account
the antibiotic sensitivity (Cifran, Ciprobay, Ciprofloxacin, Sumamed,
Rovamycine) in combination with LT based on a complex technique. After the
5th – 6th session the patients’ general well-being was improved, pain
syndrome was decreased, the inflammatory infiltrates were reduced thanks to
enhancement of local blood flow, adhesive process was resolved, and the somatic
temperature was normalized. As a result of conduct of the therapeutic treatment
courses it was noted in the patients the intensification of function of adrenal
cortex with increase of content of 17-oxyketosteroids by 7–9% that speaks for significant
activation of hormone system. The quality of follicle-stimulation hormone
increased by 2–5%,
intestinal cell-stimulating hormone by 3–6%, lactogenic hormone by 5–7%, which undoubtedly had an impact on
restoration of reproductive function of female gonads. Spermogram parameters
improved significantly: pH value of 17 patients was restored, the number of
active sperms increased, the sperm agglutination occurrences disappeared, the
content of pathogenic sperm cells reduced markedly. The treatment conducted has
resulted in impregnation in 15% of women having long-term infertility
[Dzhumaliyev S.N., 2000]. Similar data were got by I.A. Diakov
(2000).
Technique 1: ILBI using Mulat-M10 laser
therapeutic device, wavelength 0.65 µm, optical radiation power at the
light-guiding fiber output 1.5–2 mW, daily or every second day, 15 sessions per
course.
Technique 2: transcutaneous contact using
Mustang 2000 or Mustang 2000+ laser therapeutic device,
MLO1K-2000 IR-pulse
radiation probe of matrix type, wavelength 0.89 µm, pulsed radiation power
40–60 W, wavelength
80–1500 Hz, on tender
points (hepatobiliary, lumbosacral zones, the region of thyroid body and thymus
gland), exposure 30–60
sec., 7–10 sessions per
course.
Technique 3: transcutaneous contact using
Mustang 2000 or Mustang 2000+ laser therapeutic device. LO4-2000 radiation probes with
ZM50 magnetic attachments,
frequency 80–600 Hz, output
radiation power 15–17 W, on
the area of epididymis projection, exposure 30–60 sec., 7–10 sessions per course.
Technique 4: endocavitary using Mustang 2000 or Mustang 2000+ laser therapeutic device. LO4-2000 radiation probe (pulse,
wavelength 0.89 µm, frequency 80–150 Hz) and KLO3-2000 radiation probe (continuous, wavelength 0.63 µm), maximum power,
alternately, by 5 min., in 2 min., using U-1 urethral
attachment, intra-urethrally, moving from sphincter outwardly, 10–15 sessions per course.
17. Penile fibromatosis (Peyronie’s disease)
Peyronie’s disease (PD) is a deformity of penis
connective tissues which is featured by local fibrosis with change in the
collagen structure and damage of elastinic base of penis albugineous tunic
which changes gradually the anatomy of penis and can result in erectile
dysfunction [Gelbard M.K. et al., 1990; Lue T.F., 2002].
As of today, PD therapy is one of the most
challenging and contradictory problem of the modern urology that is caused in
many instances by no consensus regarding the disease progress in spite of the
achieved success in understanding of certain most important PD development
mechanisms.
The modern concept of PD pathogenesis
considers the formation of plaques in PD as a process representing by a chain
of genetic, structural and immunologic occurrences which valid reasons,
however, are not fully explored yet.
Magneto-laser therapy, included into the
complex of conservative therapy is applied in the treatment of acute stage of
disease. The operative therapy is applied during the stabilization of
indurative process in order to repair any penile deformation at
erection.
Having objectively identified the acute
stage of PD by conducting U/S-angiography or soft X-ray tomography of penis
with contrast enhancement it is recommended to conduct the third diagnostic
stage, which includes an immunoassay to the extent of examination of
Т-lymphocytes and their sub-populations (CD3, CD4, CD8) cell-bound immunity and enzyme-linked
immunoassay of antibodies to herpes simplex virus 2 (HSV-2), as well as a study of interferon profile to
the extent of analysis of virus-induced α-interferon and mitogen-induced γ-interferon for the
purpose of determining the scope of pathogenic therapy of PD acute
stage.
The mandatory components of a conservative
therapy course are magneto-laser exposure of the area of albugineous tunic
affection and vitamin E as antioxidative therapy. The scope of therapy depends
on the presence of penile deformation at erection. If the presence of erectile
deformation is detected, the complex of the conservative therapy should include
injections in the region of A-intron affection or Verapamil for stopping and
regressing the fibrosis of albugineous tunic. Moreover, it should be taken into
account that the efficiency of the treatment assessed by reduction of penile
deformation angle will depend on its value detected primarily and will be
considerably higher in case of A-intron than Verapamil.
In case if chronic HSV-2 infection is
detected it is necessary to add to the complex the treatment with the use of
injections of Verapamil anti-virus therapy that improves considerably the
efficiency of the therapy as a whole. Application of A-intron injections is not
required in case of detection of chronic HSV-2 infection, because the
preparation has a pronounced immune-modulating and antiviral activity. If
cellular immunity deficiency and/or virus-induced α-interferon and mitogen-induced
γ-interferon it is
necessary to add to the treatment course A-intron in the form of
injections in the area of affection or intramuscular with control study of
cell-bound immunity and interferon profile once per month.
U/S-monitoring studies in full standardized
scope are recommended for conduct every 4 weeks of conservative therapy to
control any change in plaque dynamic, possible appearance of the new indurative
elements, as well as to monitor fibroplastic induration activity. It is
recommended to complete the course of conservative therapy with following
obligatory supervision of the patient within a year in case if chronic stage of
disease is detected.
–
The laser therapy is carried out by contact,
stationery, with magnetic attachment. Radiation optical band – red (wavelength 0.63 µm, KLO4-2000 radiation probe (Fig. 13)),
biosynchronized modulation according to the heart and respiration rate
(BIO controller), radiation power (without modulation) – 20 mW. Magnetic static field induction
– 150 mT. Total exposure
time – 15 min. per one
session, daily, the first 2 weeks - once a day, and then 2 times per
week.
A-intron injections in the area of
albugineous tunic affection shall be made twice a week at the dosage of 1 to 3
mln. IU under the control of interferon status indices. The injections of
Verapamil in the area of albugineous tunic affection are made twice a week at
the dosage of 2.5 mg.
Monitoring ultrasound investigations of
penis with the use of U/S-angiographic methods for the purpose of assessing the
activity of indurative process shall be made once per month during the course
of therapy. Establishing a stable phase is a basis for termination of the
course of conservative therapy. On average, the course scheme of IFN therapy is
from 40 to 60 mln. IU [Ivanchenko L.P., 2007].
18. Chronic renal insufficiency
Over the years M.B. Lutoshkin (2003) has
observed a large group of patients with chronic renal insufficiency, which
treatment was carried out by conservative methods for several reasons. The
complex therapy included also LLLT action with a positive result. Lack of renal
functional reserve remained in the patients, but there was recorded the
reduction in rate of renal insufficiency progression, reduction in the level of
urea, creatinine, medium molecules in blood serum. A part of these indices had
statistically-valid differences, but only in the patients with chronic renal
insufficiency of stage I.
LT technique: ILBI using Mulat-M10 laser
therapeutic device, optical radiation power at the light-guiding fiber output
1.5–2.0 mW, duration of one
session 25–30 min,
10–12 daily sessions per
course. Repeated course of laser therapy in 6 and 12 months. Then the repeated
courses of laser therapy every 6–12 months during 5–10 years [Lutoshkin M.B. et al., 2004].
19. Chronic pyelonephritis
Pyelonephritis is the most common
infectious-inflammatory disease of the mucous membrane of the urinary tract and
tubulointerstitial tissue of kidneys. The share of pyelonephritis is more than
half of all patients with diseases of the upper urinary tract. The incidence of
pyelonephritis is closely dependent on gender and age. Women of young and
middle age suffer from this disease 5 times oftener than the men. This is due
to the anatomical and physiological characteristics of the female body. Despite
the widespread use of different groups of antibacterial drugs a growth of this
disease occurrence, disability and increased mortality are noted due to
it.
Due to the fact that chronic pyelonephritis
is the primary cause of renal insufficiency and nephrogenic hypertension,
active treatment should begin with the first days of recrudescence and continue
until elimination of all signs of inflammation. In recent years, the treatment
of chronic pyelonephritis made significant progress thanks to the introduction
in the medical practice the laser and especially magneto-laser therapy. These
treatment methods improve the microcirculation and blood rheology in the area
of inflammatory focus;
have anti-oedematous, desensitizing and immunomodulatory effects [Avdoshyn
V.P., 1992]. At the same time, laser therapy promotes the concentration of
drugs in inflammation focus and their potentiation [Andryukhin M.I.,
1992].
Laser therapy and/or MLT is carried out as a
part of a complex treatment, including antibacterial therapy, detoxification
agents, immunomodulators, antioxidants, vasoactive drugs and antihypertensive
drugs from the group of ACE inhibitors.
Evaluation criteria of treatment
effectiveness are persistent improvement of general condition and stable
improving of quality of patient’s living, the positive dynamics of clinical and laboratory study
results. The data of the studies show a pronounced positive effect of the use
of LLLT in treatment of the patients with chronic pyelonephritis in the acute
phase. It is noted not only a positive trend of certain clinical and laboratory
signs, but also a decrease in the length of stay of the patients in bed of an
in-patient facility. Attention should be also paid to the fact that the
patients receiving treatment course of LLLT have significantly less recurrences
of acute pyelonephritis after passing both first and repeated courses of
preventive MLT courses.
V.R. Sultanbayev (1993) recommends carrying
out of ILBI for the patients with chronic pyelonephritis that is conditioned by
optimization effect of LLLT on the antioxidant system.
Laser therapy course consists of 12-14 sessions once daily. The first 5-6 sessions
– ILBI with radiation power
of 1.5-2.0 mW, exposure time of 25-30 minutes. Then, a transcutaneous
irradiation of the projection of the kidneys by pulsed IR-laser radiation
(pulsed power of 6.4 W, frequency - 1500-3000 Hz, exposure 4 minutes per zone).
During 1 session, action on 2-3 zones of the front, a middle and posterior
axillary line is made. The induction of magnetic field is 50 mT. The patient
lies on his side with underlying cushion. Two laser radiation probes of
LO4-2000 type are applied
simultaneously.
For the patients with syndrome of
hypertension, additionally radiation of zones located paravertebral at the
level of CIII–ThIII right
and left simultaneously by two LO4-2000 radiation probes is conducted, 4-6 W pulsed power, frequency
80-150 Hz. Exposure of one field - within 1 minute. MLT course is repeated in 2
months and the third course – in 3 months after the second. In the future, the annual preventive
course of MLT shall be carried out [Lutoshkin MB, 2003; Slastnikova EB,
1994].
| 