1. Historical Aspects of Photodynamic Therapy Development
Alexander А. Radaev
The “Magic Ray” Moscow Center of Laser Medicine, Moscow, Russia
Photodynamic therapy (PDT) uses the local activation of a photosensitizer accumulated in a tumor by means of light. In the presence of tissue oxygen, this activation brings about a photochemical reaction that destroys tumor cells. The PDT mechanism can be described as follows:
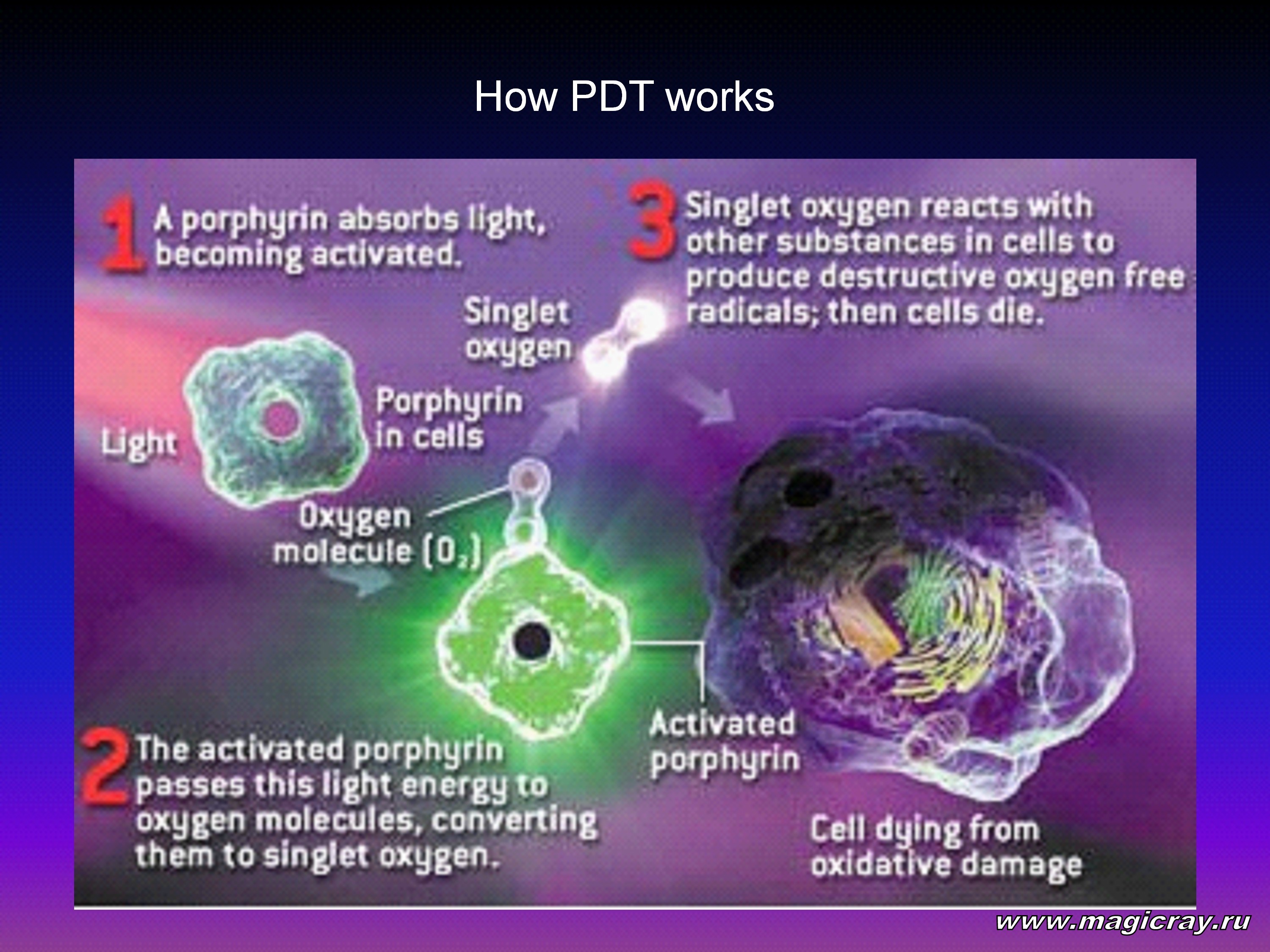
When a photosensitizer molecule absorbs a quantum of light, it goes to an excited triplet state. The excited molecule can undergo photochemical reactions of two types. In the first type, the molecule reacts directly with biological molecules. This leads to the generation of free radicals. In the second type, an excited photosensitizer molecule reacts with an oxygen molecule. As a result, singlet oxygen is produced. This substance is a strong oxidant, which is cytotoxic in action.
Soon after its development, the photodynamic effect was used in oncology. It proved to be beneficial in the treatment of cancer. It also appeared to be effective in the treatment of many nonmalignant diseases.
Presently, thousands of scientists and clinical practitioners are studying different aspects of PDT and PDT-related fluorescent diagnostics. By now, PDT has been applied to tens of thousands of cancer patients. The results obtained opened up new prospects for PDT. Now, much interest is shown to the history of PDT, which has matured into a large area of photomedicine.
The history of modern PDT goes back to the attempts of ancient Egyptians to treat skin diseases with light-absorbing compounds. Six-thousand-year-old annals tell us that ancient Egyptians applied vegetable substances to produce photoreactions in tissues. The substances were employed in the treatment of depigmented skin lesions (vitiligo). These lesions used to be regarded as manifestations of leprosy. Egyptians utilized natural photosensitizers - psoralens. They were contained in many plants such as the parsnip, parsley, and Saint-Join’s-wort. Egyptians made a powder of these plants and applied it to depigmented skin lesions. After that, the person was exposed to bright sunlight. The sunrays activated the applied photosensitizers. As a result, the lesions became pigmented. This effect was similar to a sunburn.
Photomedical procedures were also described as far back as 1550 B.C. We learn about them from the Ebers papyrus [1] and the holy Indian Book Atharva Veda [2]. At that time, phototreatment was indicated mainly to people with depigmented skin lesions. People thought that these lesions were caused by leprosy, not by vitiligo (leukoderma). Ancient Indian books describe the application of black seeds of
Beivechi (Veisuchaika), followed by their exposure to direct sunlight. Later, Beivechi was identified as Psoralena corylifolia (Rapinat Herbarium, India, 1982). This plant contains psoralens (furocumarins), which are anaerobic photosensitizers. Beivechi was mentioned as a remedy for vitiligo in Buddhistic books written in A.D. 200 and in Chinese books written in the 10th century A.D. In his famous book Mofradat Al Adwiya (the 13th century A.D., Egypt), Ibn El Bitar described the treatment of depigmented skin lesions (vitiligo) with a tincture of honey and powdered Aatrillal seeds [3]. Aatrillal is a plant that was abundant in the Nile valley. Later, Aatrillal was classified as Ammi majus - a plant that contains many psoralens. This plant was applied not only topically. It was also administered orally. In the latter case, the patient had to lick off a mixture of honey and powdered Ammi majus seeds. After that, he or she sat in the bright sun for an hour or two. The sunrays were incident on depigmented skin lesions and activated psoralens. This brought about a photodynamic reaction and vesiculation (the formation of blisters). In the case of leukoderma, vesiculation caused reepithelization and repigmentation.
Furocumarins contained in plants make the skin photosensitive. They also stimulate the production of pigment melanin in the skin. This favors the recovery of skin pigmentation. Presently, Ammi majus is used to produce an ammifurin compound. It contains a mixture of three furocumarins: isopimpinelline, bergapten, and xanthotoxin. This compound is employed in the treatment of vitiligo, psoriasis, neurodermite, and lichen ruber planus.
Psoralens were actively investigated in Egypt over the past century. Active ingredients were extracted from plants to be assayed [3]. It was found that 8-methoxypsoralen was the most important compound. Soon afterwards, it was applied in the psoriasis treatment. Psoralens can bring about photosensitization and photochemical reactions in the absence of oxygen.
Oxygen-dependent photodynamic reactions were discovered by Oscar Raab in winter of 1897 to 1898.
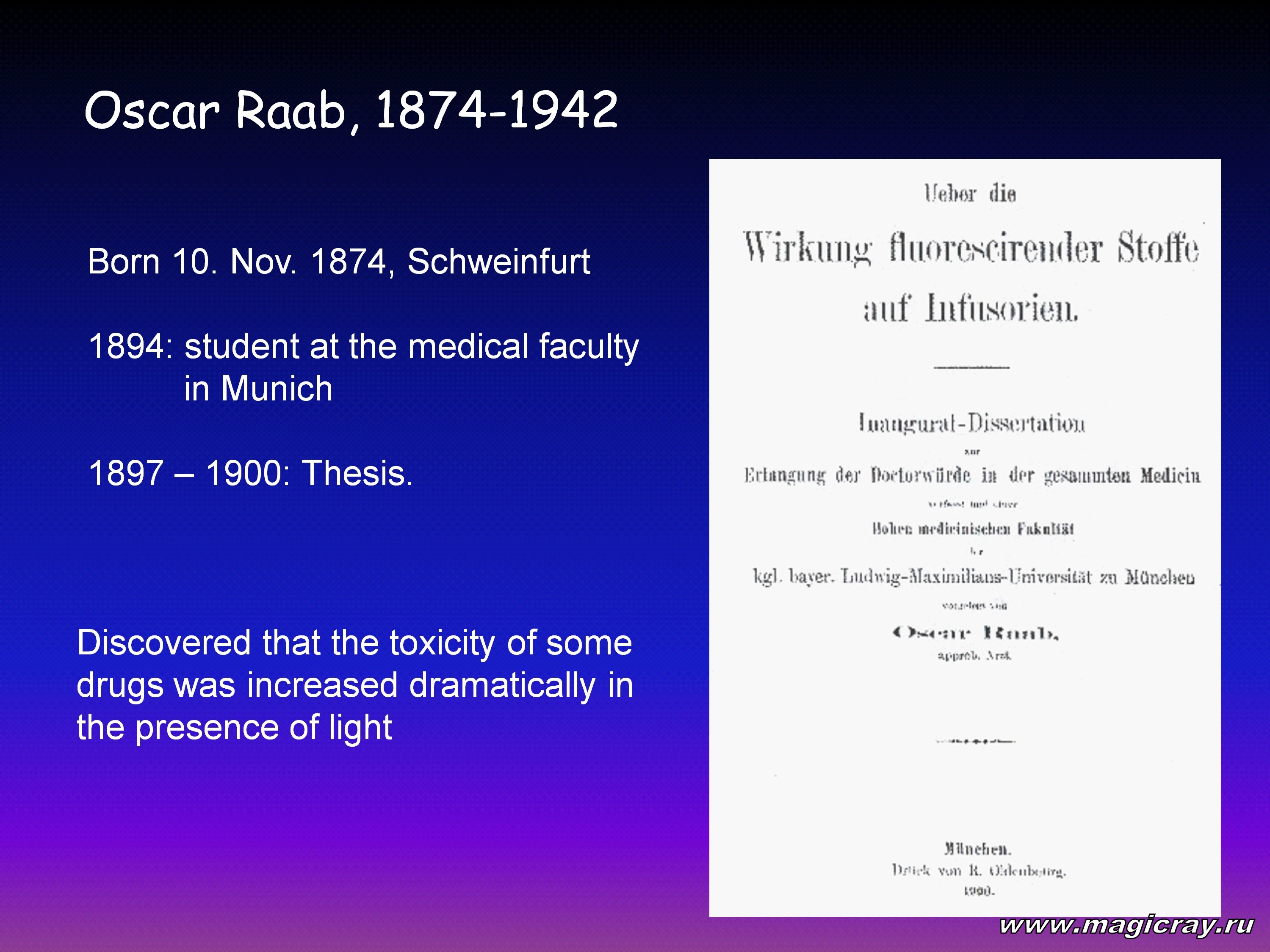
Oscar Raab was a student at the medical faculty of the Pharmacological Institute of the Munich University. He did research under the guidance of Professor Hermann von Tappeiner and experimented with paramecia influenced by light and dyes (such as acrydine) [4, 5].
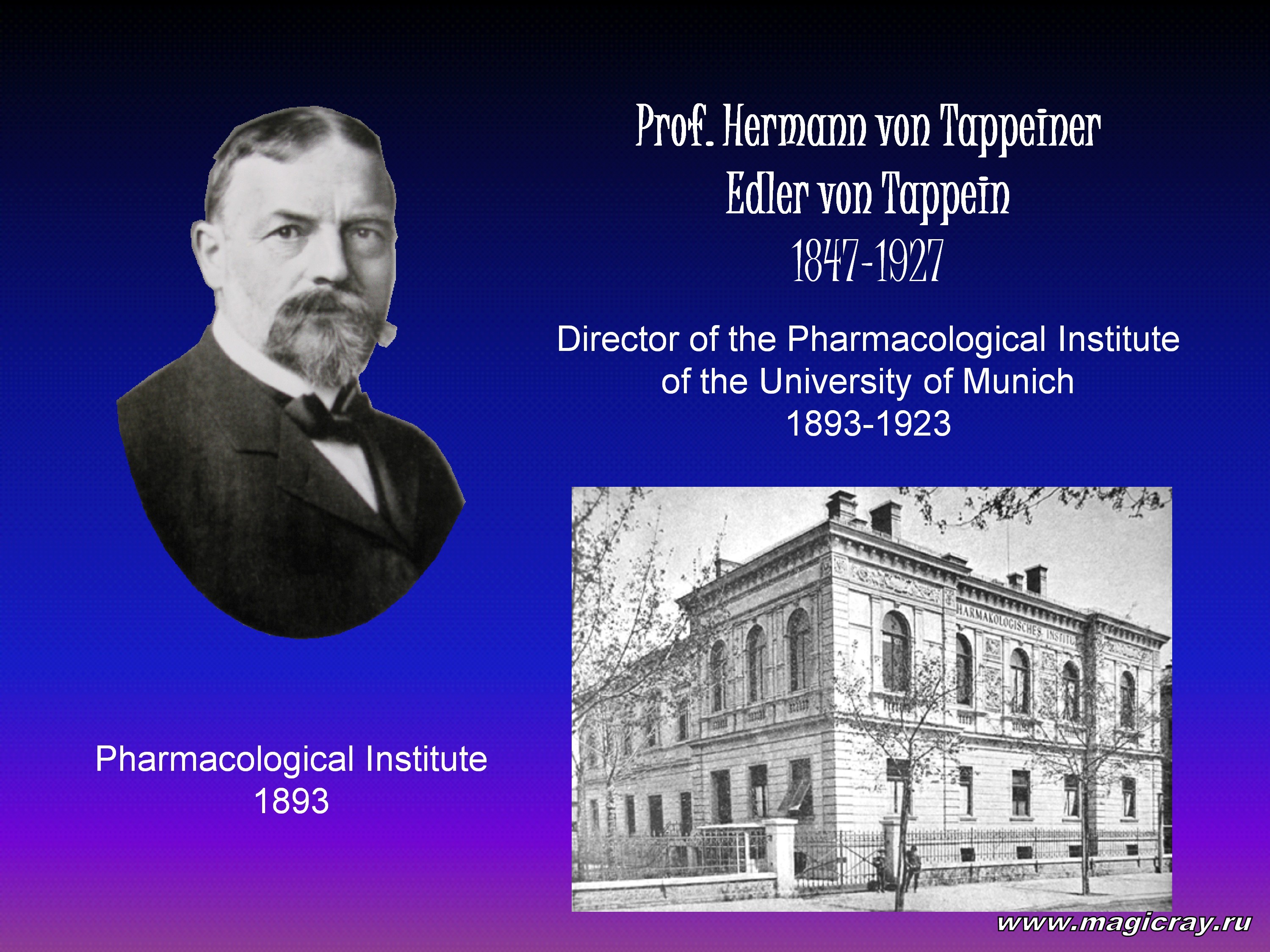
Oscar Raab noted that an acrydine solution killed paramecia upon irradiation with light. There was no such effect observed in the absence of light. This finding gave rise to two questions. First, has the acrydine solution imparted toxic properties to light (for example, by means of absorption of a wavelength that is vital for life)? Second, has light transmuted the acrydine dye into a toxic agent? The first hypothesis was rejected after an experiment in which paramecia remained alive when they were placed in an undyed solution and exposed to light that passed through an acrydine solution, which served as a filter. In other words, the acrydine dye did not transmute light into toxic radiation. However, the acrydine dye had some specific properties such as absorption and fluorescence. Since absorption did not make the light toxic, fluorescence was thought to be the major damaging factor. Oscar Raab hypothesized (probably, with a hint of his chief - Professor H. Tappeiner) that fluorescing substrates, such as the acrydine dye, should convert the energy of light into an active (living) chemical energy, which kill paramecia. The active chemical energy formed the basis for photodynamic therapy. On the basis of a new knowledge about photodynamic effects, in 1903 Hermann von Tappeiner and Albert Jesionek performed the first PDT session in a patient with skin carcinoma, as a photosensitizer, eosin was used [6].
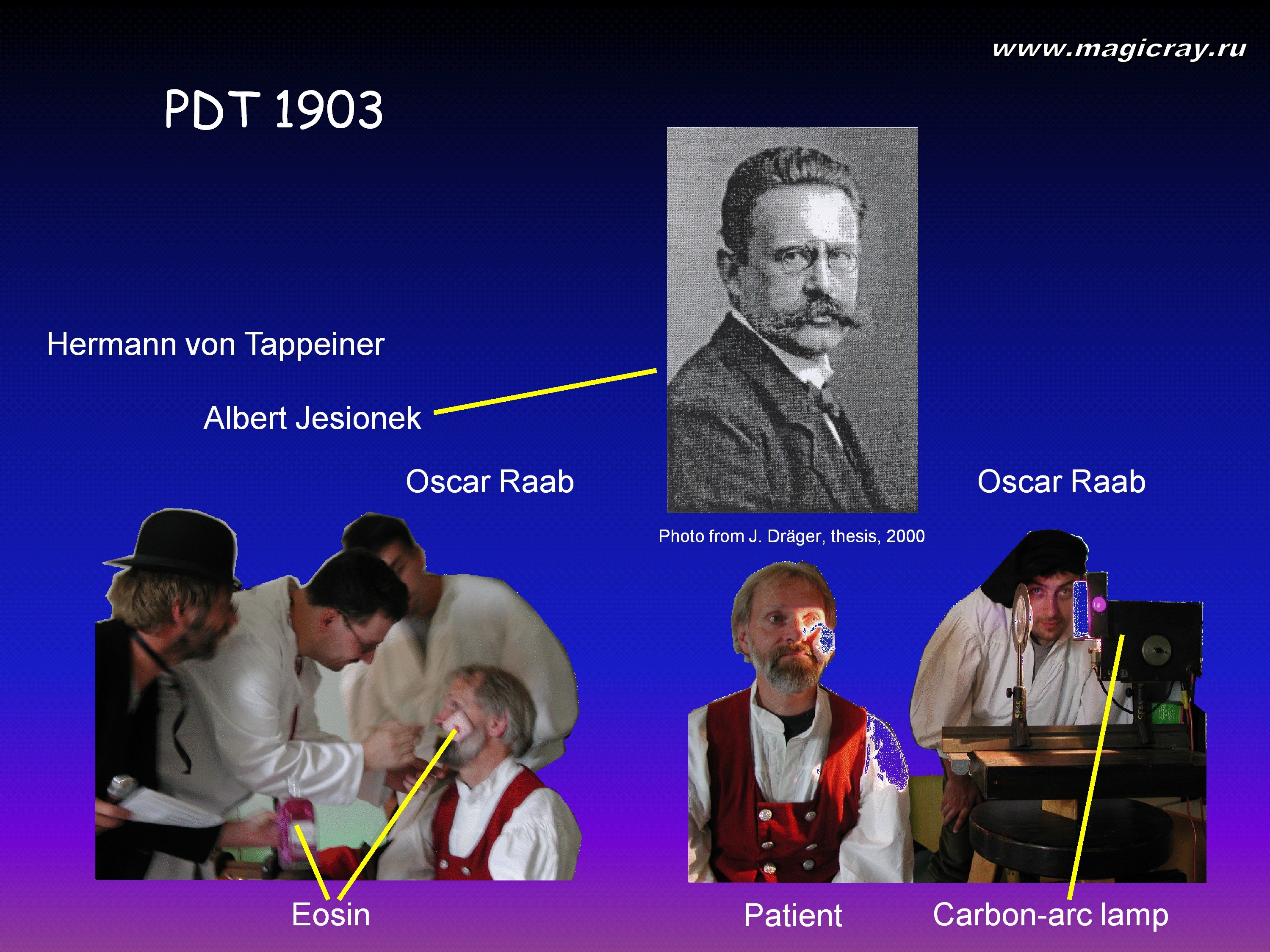
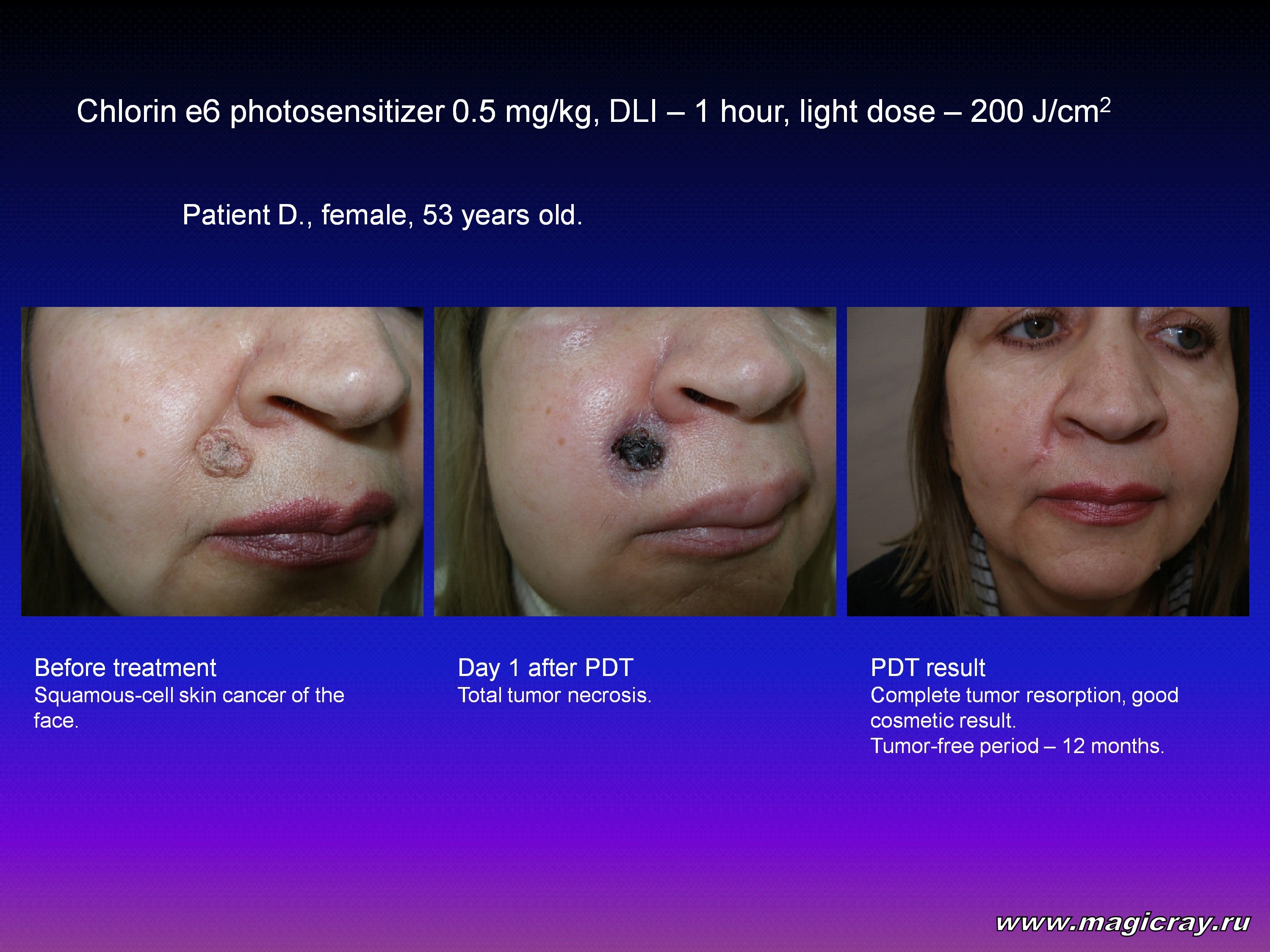
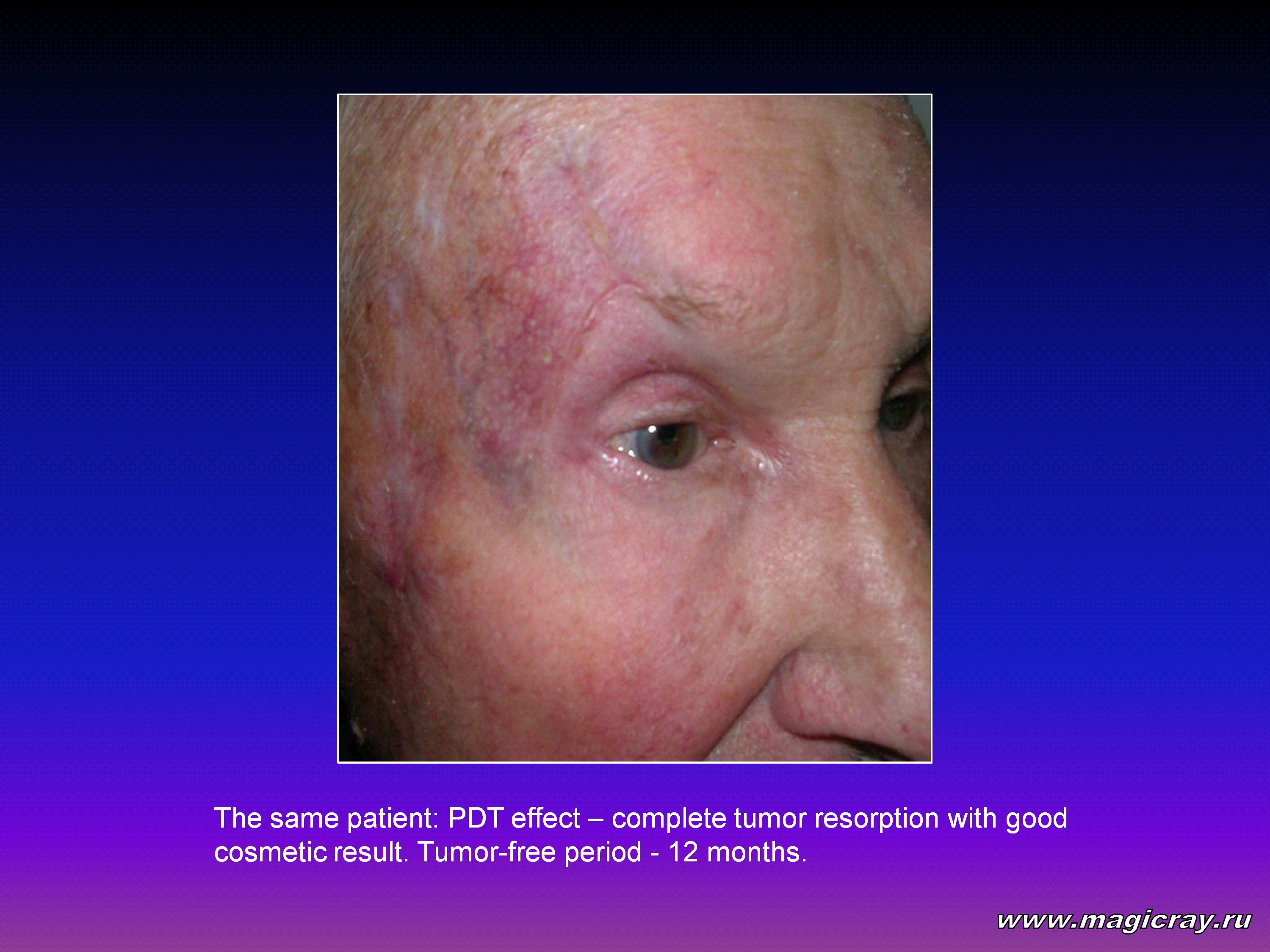
In 1905, these scientists described the results of their first treatment of 6 patients with a facial basal-cell carcinoma. The treatment was performed using a 1-percent eosin solution and a long-term exposure either to the sunlight or to carbon arc-lamp light [7].
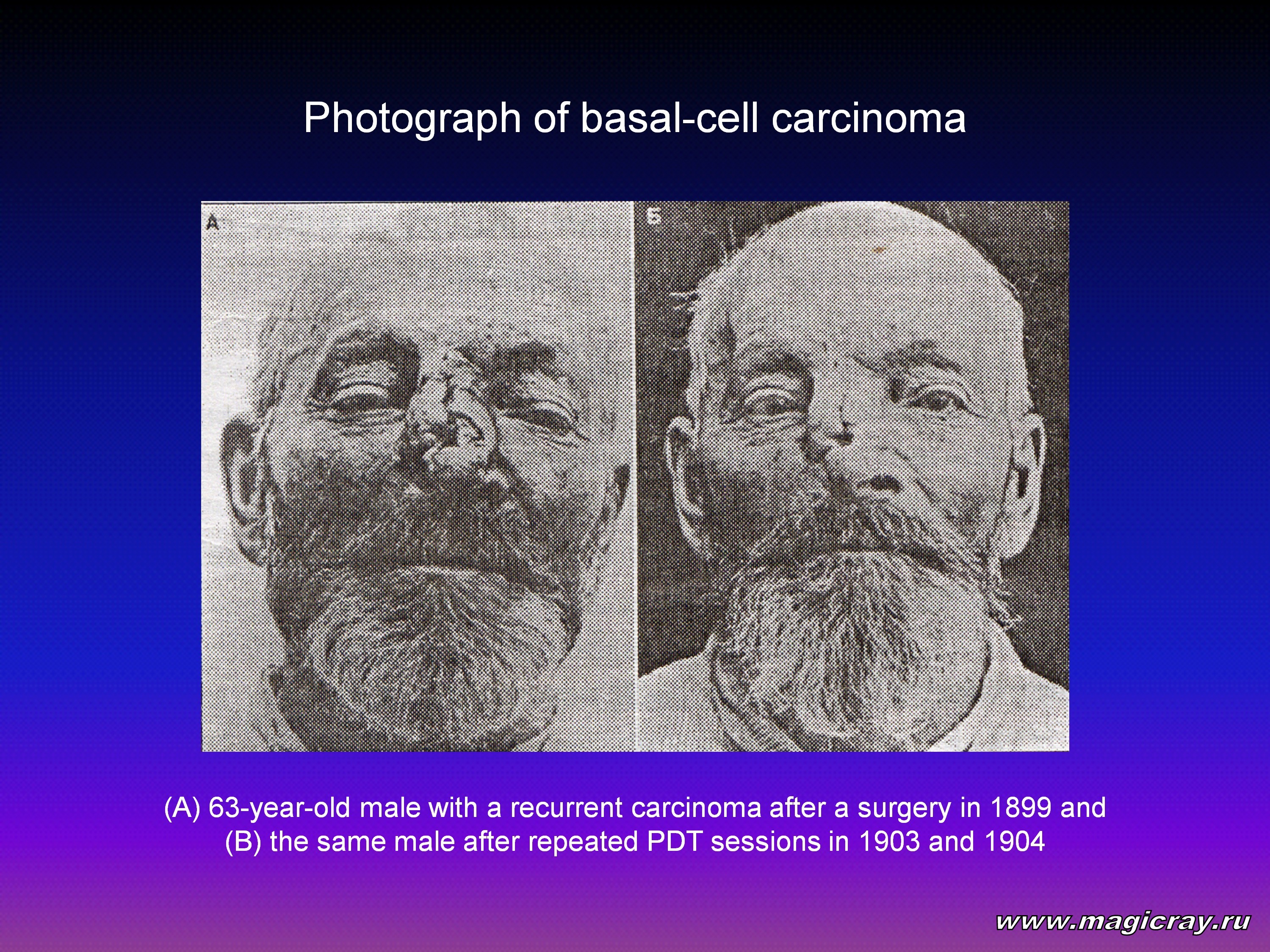
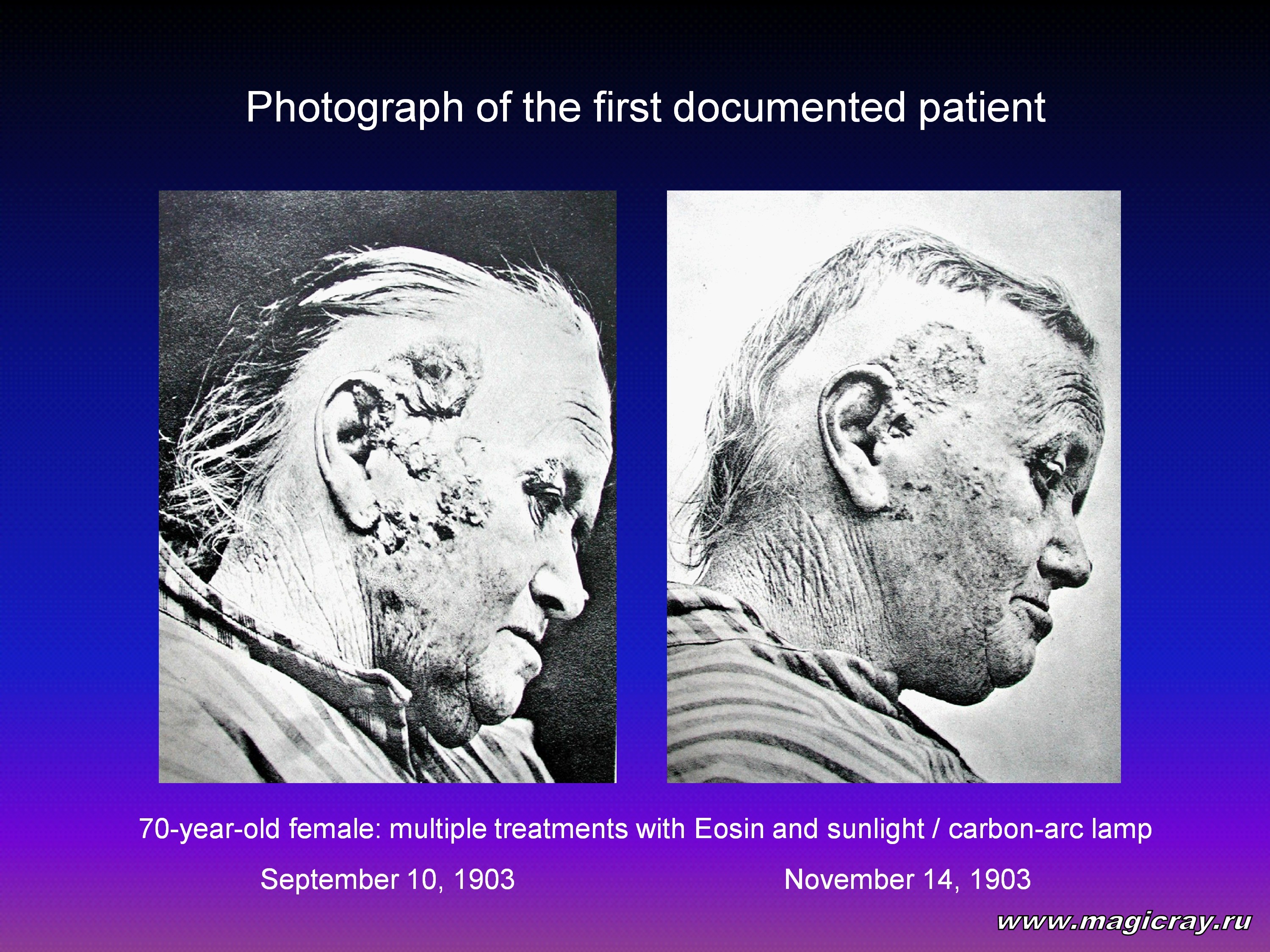
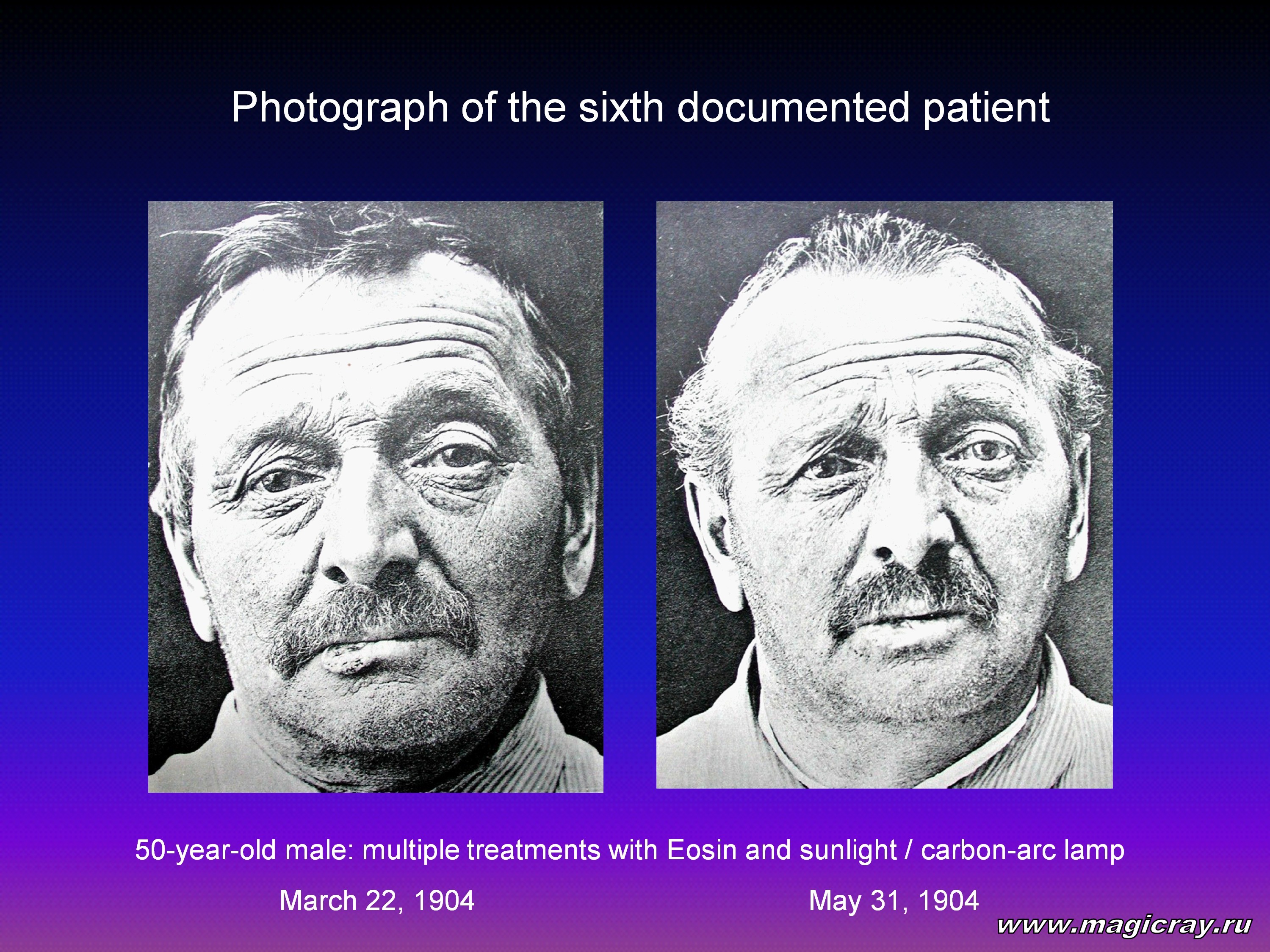
As a result, 4 patients showed complete tumor resorption. A tumor-free period was equal to 12 months. At the same time, H. Tappeiner and A. Jodlbauer [8] coined the term photodynamic action (“photodynamische wirkung”). Walter Hausmann started his first experiment on hematoporphyrin phototoxicity in 1908.
He established that hematoporphyrin was an active photosensitizer for paramecia and erythrocytes [9]. Shortly before 1910, Walter Hausmann made unorthodox experiments on white mice. The mice were injected hematoporphyrin, which was followed by their exposure to sunlight. The mice showed reactions that depended on the photosensitizer and light doses [10]. Walter Hausmann hypothesized that the primary PDT effect was associated with the damage of peripheral vessels.
Friedrich Meyer-Betz was the first to study the hematoporphyrin effect on the human subject [11]. He performed his experiment on himself.
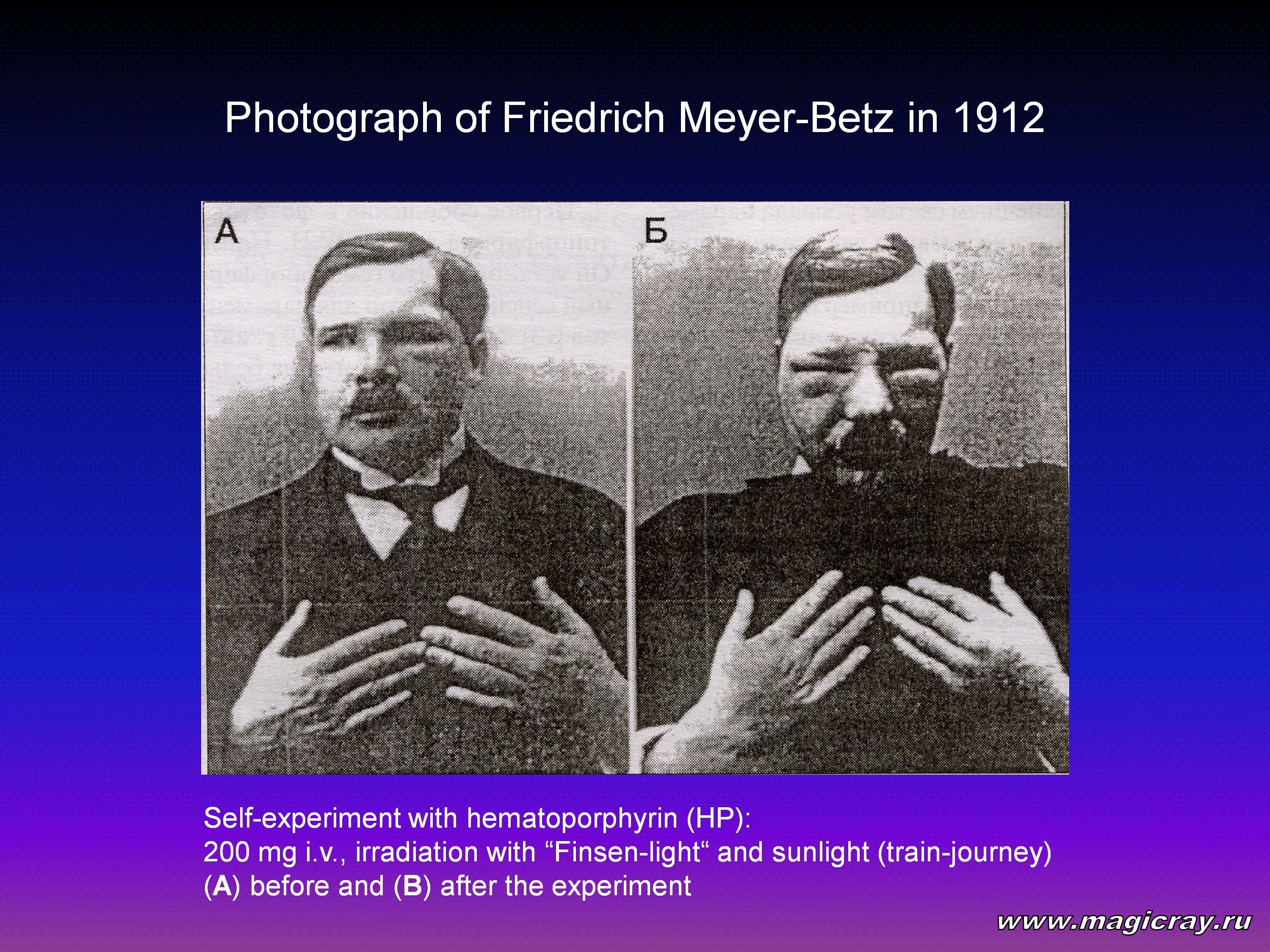
On October 14, 1912, he made an intravenous self-injection of 200 mg of hematoporphyrin. After that, he exposed himself to the sunlight to demonstrate photosensitivity. The sunrays caused an edema and hyperpigmentation, which persisted for 2 months. Further investigations confirmed that a systemic hematoporphyrin administration produces a violent photosensitization of various tissues, the cutaneous ones included.
In 1924, A. Policard revealed diagnostic capabilities of hematoporphyrin fluorescence [12]. He observed that ultraviolet radiation excited red fluorescence in the sarcomas of laboratory rats. A. Policard hypothesized that fluorescence was associated with endogenous hematoporphyrin accumulation. He related hematoporphyrin accumulation with the secondary infection of hemolytic bacteria.
In other experiments with rats, the injection of exogenous hematoporphyrin intensified red fluorescence of neoplastic tissues [13]. This occurred because tumors accumulated hematoporphyrin more actively than healthy tissues. As a result, new diagnostic and therapeutic applications of photosensitizers were developed.
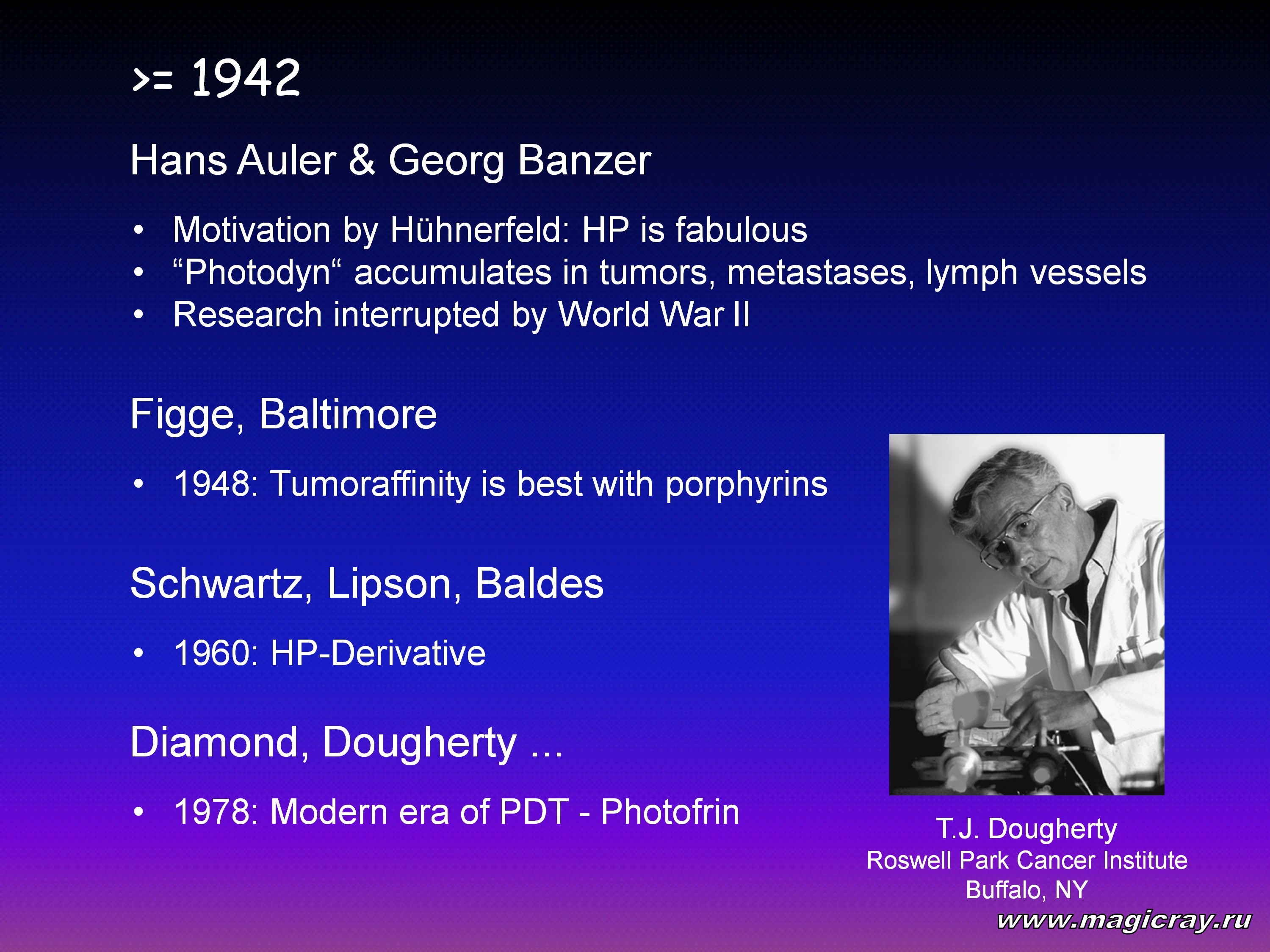
In 1948, F. H. J. Figge with co-workers [14] showed on laboratory animals that porphyrins exhibited high affinity to rapidly dividing cells (such as malignant, embryonic, and regenerative cells). Because of this, they proposed that porphyrins should be used in the treatment of cancer.
In 1954, hematoporphyrin was injected intravenously to a group of 11 patients with cancer. Hematoporphyrin was injected at doses of 300 to 1,000 mg 12 to 72 hours before the surgery [5]. During the operation, the tumor was exposed to ultraviolet A. The irradiation excited bright fluorescence in the red. It was proposed that hematoporphyrin should be used to reveal invisible tumors and determine their size during surgeries. This photodynamic approach can also detect small lymphatic nodes.
Photodynamic therapy took a giant step forward after the development of an improved photosensitizer - hematoporphyrin derivative (HpD). The point is that the hematoporphyrin itself was a mixture of porphyrins and inert impurities [15]. Hematoporphyrin derivative appeared to be twice as toxic as the original compound. It produced a twofold photodynamic effect. S. Schwartz was the first to produce HpD by processing hematoporphyrin with concentrated sulfuric and acetic acids. In 1960, he applied HpD to diagnose tumors at the Mayo Clinic [16].
In 1960, R. L. Lipson and E. J. Baldes [16] injected HpD intravenously to 15 cancer patients. Hematoporphyrin derivative was administered at a dose of 2 mg per kg of the patient’s weight. It was injected about 3 hours before the endoscopic procedure. When the fluorescent-excitation light intensity was sufficient, endoscopy gave neither false-positive nor false-negative results. It was proposed that systemic HpD administration followed by endoscopic control should be employed to diagnose malignant tumors.
In another study, HpD was injected intravenously to 226 patients. The results obtained showed that fluorescence correlated with squamous-cell carcinoma and adenocarcinoma in 75 to 85 percent of the cases. Fifty-three nonmalignant tumors produced false-positive reactions in 23 percent of the cases [17].
Investigations performed were focused mainly on fluorescent diagnosis. The first investigation of photodynamic destruction of malignant tumors by means of HpD injection was described in 1966 [18]. R. L. Lipson with co-workers harnessed the potential effect of selective destruction of tumors containing HpD. The destruction was performed due to the HpD photodynamic properties. The investigation was performed in a female patient with an extended recurrent ulcerated breast cancer. Hematoporphyrin derivative was injected repeatedly to the patient. The tumor was exposed to xenon-lamp light that had passed through a filter (the radiation spectrum is unknown). The results obtained were reported at the Ninth International Cancer Congress in Tokyo in 1966 [18].
In another study, the photodynamic effect was used to destroy gliomas, transplanted subcutaneously to rats. The animals were made an HpD injection, which was followed by their exposure to white light [19].
J. F. Kelly and M. E. Snell [20] implanted 11 malignant tumors of the human bladder into immunosuppressed mice. After that, the mice were made an HpD injection. Twenty-four hours later, they were exposed to white light. The exposure caused a pronounced tumor destruction. The authors proposed that PDT should be used in the treatment of superficial transitional cell carcinoma of the bladder of human subjects. The next year, these researchers applied HpD in the treatment of a patient with a recurrent superficial anaplastic carcinoma of the bladder. Forty-eight hours after the treatment, they observed several necrotic papillary tumors. The healthy areas of the mucous membrane of the bladder looked undamaged.
In 1978, T. J. Dougherty with co-workers [21] applied HpD PDT in the treatment of cancer patients. They treated 113 cutaneous or subcutaneous malignant tumors. The researchers observed a complete or partial resorption of 111 tumors. Extended or pigmented tumors required large HpD doses. To avoid damaging of the normal skin, they needed either to decrease light doses or to increase the time interval between photosensitizer injections and light exposures. The researchers believed that the laser should be a good alternative to arc lamps. With this end in view, they employed a tunable dye laser with argon pumping. Laser radiation was delivered via light-guiding fibers [22]. In the authors’ opinion, an essential advantage of the laser was that it enabled the use of flexible fibers.
Later (in 1980), the red laser irradiated small foci of endobronchial carcinoma. The radiation was delivered via flexible light-guiding fibers made of quartz. The fibers were inserted into the tool channel of a flexible bronchoscope [23].
It was found much later that HpD is composed of unpurified porphyrins, many of which remain inactive or show poor photodynamic activity. An HpD mixture contains 20 percent of hematoporphyrin, 25 percent of monodehydrated hematoporphyrin products (such as hydroxyethyl-vinyldeuteroporphyrin), and 5 percent of didehydratedn protoporphyrin products [24, 25]. The rest of the mixture contains porphyrins, which are united by ether bonds into complexes of 2 to 8 pyrrol rings. It is these compounds that are responsible for the biological activity of HpD. They can be separated from other components by means of various chromatographic techniques.
A compound that contains at least 80 percent of these active fractions is known as Photofrin II, Porfimer Sodium, or Dihematoporphyrin Ether (DHE) [26]. The U.S. Food and Drug Administration (FDA) has approved clinical trials of this compound. Photofrin II has already passed the third phase of clinical trials, which were sponsored by manufacturing companies Photomedica, Inc. (NJ, USA), Quadra Logic Technologies (Vancouver, Canada), and American Cyanamid Lederle Laboratories (NY, USA). This compound showed good results in PDT of different malignant tumors. Currently, Photofrin II is the most widespread photosensitizer around the world. It is dubbed the “PDT dray horse”. When injected to laboratory animals, Photofrin II is accumulated by all organs and tissues of the reticuloendothelial system (such as the liver, kidney, and spleen). It is also accumulated by tumor cells - at lower concentrations, however [27]. Tumor cells retain Photofrin II for a longer time, as compared to healthy tissues (for example, it was retained in rats for up to 12 weeks). Because the skin holds the photosensitizer, patients should remain heliophobic for 4 to 6 weeks. This is needed to avoid sunburns.
Photohem is a complete analog of Photofrin II in Russia. It was created at the M. V. Lomonosov Moscow State Academy of Fine Chemical Technology in 1990. The Photohem development was headed by Professor A. F. Mironov. Photohem is a mixture of monomeric and oligomeric hematoporphyrin derivatives. It is odorless, and it dissolves in aqueous solutions of sodium hydrate, dimethylsulfoxide (DMSO), and acetic acid. Photohem is partially soluble in ethyl alcohol. It is almost insoluble in water, chloroform, and diethyl ether. Photohem is produced from animal and human blood using an unorthodox technique. A Photohem solution mixed with a DMSO, acetic acid, and toluol in a 1:1:1 proportion shows absorption maxima at 396, 504, 570, and 633 nm. When Photohem absorbs radiation, it goes to an excited state. After that, it either fluoresces or brings about phototoxic reactions in tumor cells. As a result, it can be used both for tumor detection and destruction.
Photohem is a dark-brown powder, weighing 260 mg. It comes in sterile 50-ml vials. To make a working solution, the vial is wrapped in light-tight paper. After that, 40 ml of a sterile physiological solution are added. Then, the vial is shaken and held for 3 to 5 min to let the foam settle down. A Photohem concentration should be 0.5 percent (i. e., 5 mg of Photohem are diluted in 1 ml of the solution). A necessary dose is calculated from the patient’s weight. The Photohem solution is injected intravenously in a drip-feed or jetting manner. The patient should be in a lying position.
Photohem was first tested clinically from February 1992 to 1996. It was called a success by several Moscow Research Institutes. So, the Ministry of Health of Russia approved Photohem for a wide clinical use. By now, more than 1,500 patients have undergone PDT with Photohem. A pronounced therapeutic effect was observed in 91 percent of the patients. Of these, 62 percent showed a complete tumor resorption, whereas 29 percent showed a partial tumor resorption (the tumor halved in size in them). Early-diagnosed tumors disappeared completely in 92 percent of the patients.
In 1994, Russia launched clinical trials of Photosense — the second-generation photosensitizer. Photosense was developed in the “NIOPIK” Moscow Science-and-Development Association. The photosensitizer development was headed by Professor G. N. Vorozhtsov.
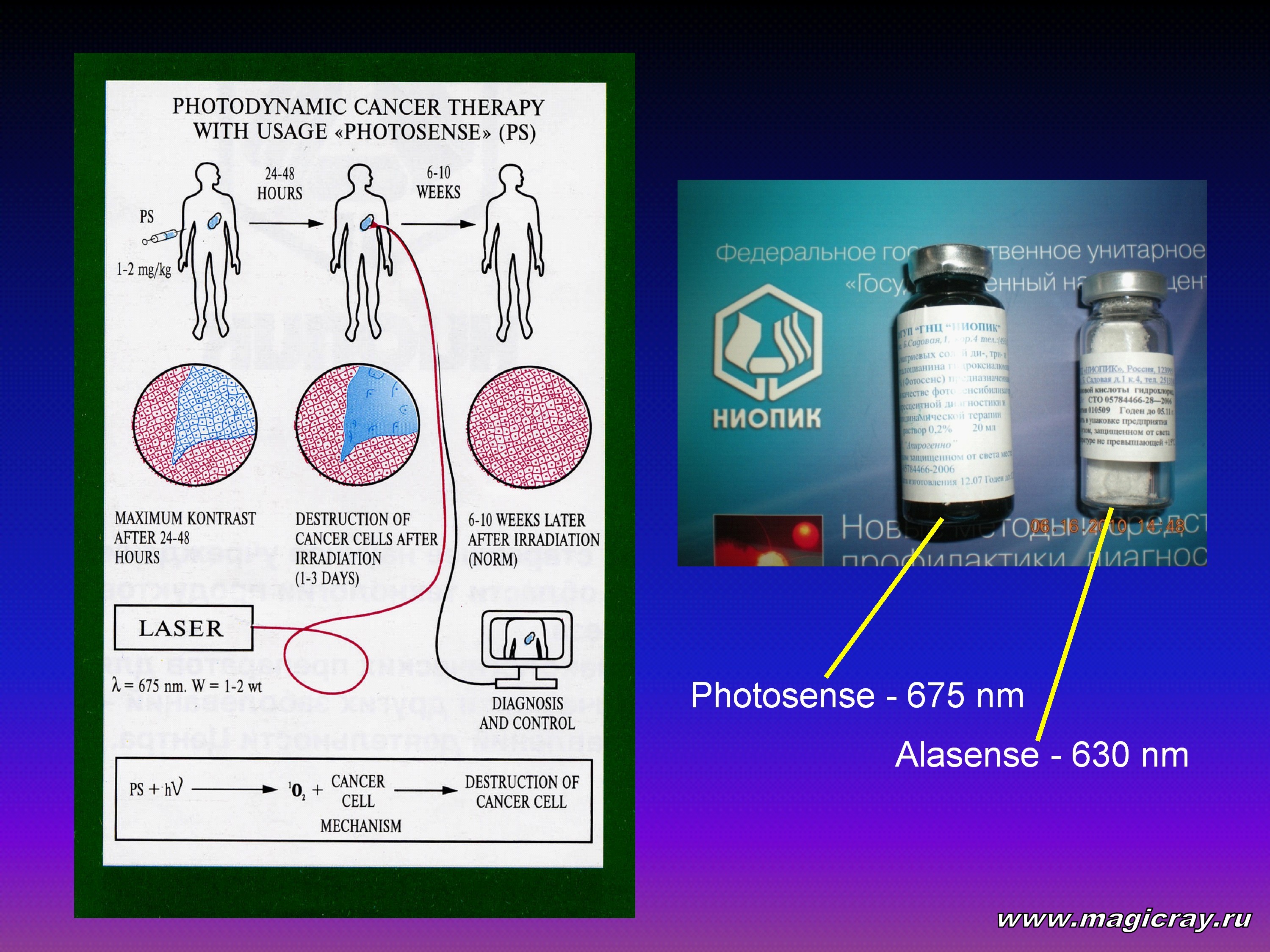
Photosense is a distilled-water solution of sodium salts of aluminum sulfonated phthalocyanine. It may contain from di- to tetra-substituted phthalocyanines. Photosense is a transparent and odorless solution. It is blue-turquoise in color. Photosense has strong absorption in the red region. A water Photosense solution shows maximum absorption at 675 nm. It also has a weaker absorption at 350 nm. Photosense offers some advantages over HpD photosensitizers. First, it shows a higher photodynamic activity in the red region. Second, it is activated by optical radiation that penetrates biological tissues deeper. As a result, Photosense can be employed to treat deep tumors. Photosense is injected under dark-room conditions. It is injected intravenously in a drip-feed or jetting manner. Before the injection, Photosense is thinned with a sterile isotonic sodium-chloride solution in a 1:4 proportion. A single dose ranges from 1 to 2 mg per kg of the patient’s weight. Photosense is injected 24 – 48 hours before tumor irradiation. The patient should remain heliophobic for 4 to 6 weeks after treatment. Photosense comes in 50-ml glass vials as 0.2-percent injection solution. At present, Photosense is being tested at several Moscow Research Institutes. It passes the third phase of clinical trials. Photosense is employed in PDT of malignant tumors. It is also used in the treatment of severe festering wounds, trophic ulcers, and some other nonmalignant maladies.
Over the past ten years, much interest has been shown to tetrapyrrol compounds (such as chlorophyll derivatives). These substances were tested as photosensitizers in the PDT of malignant tumors.
The main problem was to increase the selectivity of photosensitizer accumulation in tumors. Poor selectivity resulted in poor therapeutic efficiency. It also brought about hypersensitivity of the patient’s skin to daylight.
Tetrapyrrol structural and functional features made it possible to synthesize compounds with specified properties. As a result, new PDT photosensitizers were built and produced. Such photosensitizers showed higher tumor tropism and higher cytotoxicity to tumor cells. Having analyzed much experimental and clinical data, researchers specified main requirements to an optimum photosensitizer. These requirements included photophysical, chemical-engineering, as well as biological (such as toxic and pharmacokinetic) criteria. Some of the criteria are as follows:
- low toxicity at therapeutic doses in darkness,
- highly tumor-targeting accumulation,
- fast elimination from the skin and epithelium,
- absorption peaks in the low-loss transmission window of biological tissues (the far-red and near-infrared bands),
- optimum ratio of the fluorescence quantum yield to the interconversion quantum yield (the former parameter determines the photosensitizer diagnostic capabilities, it plays a key role in monitoring the photosensitizer accumulation in tissues and its elimination from them; the latter parameter determines the photosensitizer ability to generate singlet oxygen),
- high quantum yield of singlet oxygen production in vivo,
- available manufacturing and synthesis,
- homogeneous composition,
- high solubility in water, injection solutions, and blood substitutes, as well as
- storage and application light stability.
A serious PDT drawback was the limited penetration depth of laser radiation. Clinical photosensitizers have maxima of photodynamic action at 620 to 690 nm. In this range, optical radiation penetrates biological tissues poorly (at a depth of several millimeters). Maximum penetration lies in the far-red and near-infrared bands - from 750 to 1,500 nm. Many commercial lasers operate in these ranges. Hence, we need photosensitizers that would effectively generate singlet oxygen in these ranges. They will considerably widen PDT application.
Such photosensitizers are actively sought among chlorin, bacteriochlorin, purpurin, benzoporphyrin, texaphyrin, etiopurpurin, naphthalocyanine, and phthalocyanine derivatives. Special interest is shown to photosensitizers that can be both rapidly accumulated and decomposed. One day, a bank of tumor-targeting photosensitizers will be created (as it has been done for tumor chemotherapy). Such tumor-targeting photosensitizers will be effective for specific nosological and histological forms of cancer.
E. Snyder (USA) was the first to suggest in 1942 that water-soluble chlorophyll derivatives should be used for medical purposes. Chlorin mixtures were composed mainly of chlorin p6. They were administered orally or intravenously. These compounds were nontoxic, hypotensive, antisclerotic, spasmolytic, anesthetic, and antirheumatoid in action. They also produced a favorable effect on biochemical indices of blood. Their daily oral administration at a dose of 1 g for 30 days decreased the cholesterol count of blood by a factor of 1.5 to 2. Due to this, water-soluble chlorins were employed to prevent and treat cardiovascular diseases, atherosclerosis, and rheumatoid arthritis.
Pheophorbid A derivatives were the first chlorin-type derivatives used in PDT. In 1984, some of them were patented in Japan as potential photosensitizers for PDT.
The application of chlorin-type derivatives in PDT was reported in 1986. A research team from the U.S., which included J. Bommer, Z. Sveida, and B. Burnham, analyzed mono-L-aspartyl chlorin e6 (MACE) properties. This compound showed good tumor tropism and strong absorption in the far-red band. It thus met the most vital PDT requirements. This compound was put to tests in Japan, and now it passes the final stage of clinical trials. J. Bommer and B. Burnham, working with the Nippon Petrochemicals Company (Japan), filed a U.S. patent for some functional derivatives of chlorin e6 and bacteriopheophorbid A.
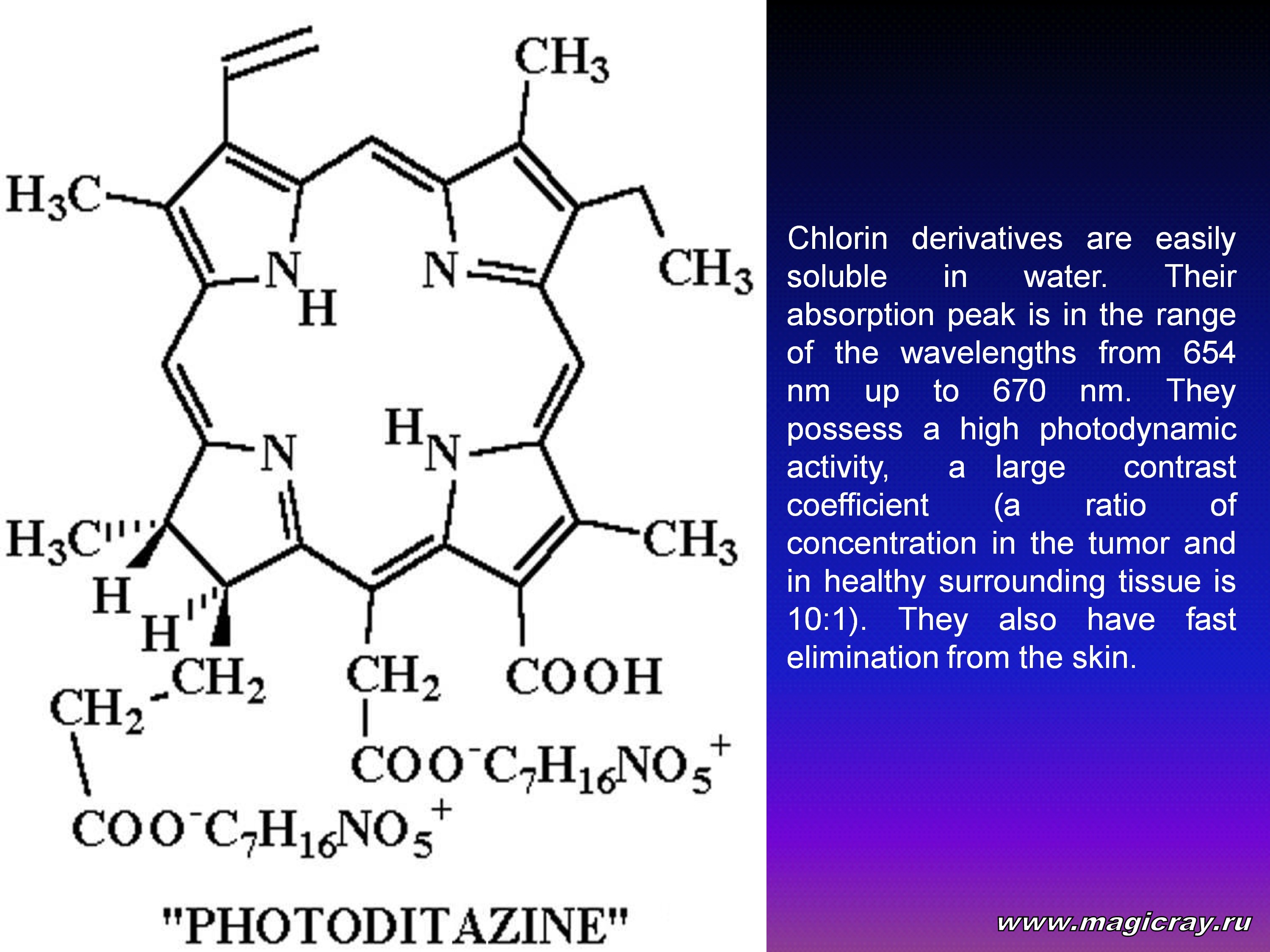
From 1994 to 2001, Russia carried out comprehensive investigations of tetrapyrrol chlorin-type macrocycles (chlorophyll A derivatives). It has to establish the structural and functional features of their accumulation in tumors. It also needed to increase PDT efficiency and to create chlorin-type drugs. At that time, scientists developed a technique for extracting biologically active chlorins from plants. Plant chlorins were found to mainly contain chlorin e6. As a result, photosensitizers of the second generation were created. They were named Radachlorin and Photoditazine (Fotoditazin™).

These photosensitizers come correspondingly as 0.35-percent and 0.50-percent solutions for intravenous injections. They are composed of three cyclic chlorin-type tetrapyrrols with a hydrogenated ring D. Chlorin e6 is their main component. It accounts for 80 to 90 percent of the mixture. Radachlorin and Photoditazine are activated by optical radiation at wavelengths of 654 to 670 nm. This radiation can penetrate biological tissues at a depth of about 7 mm.
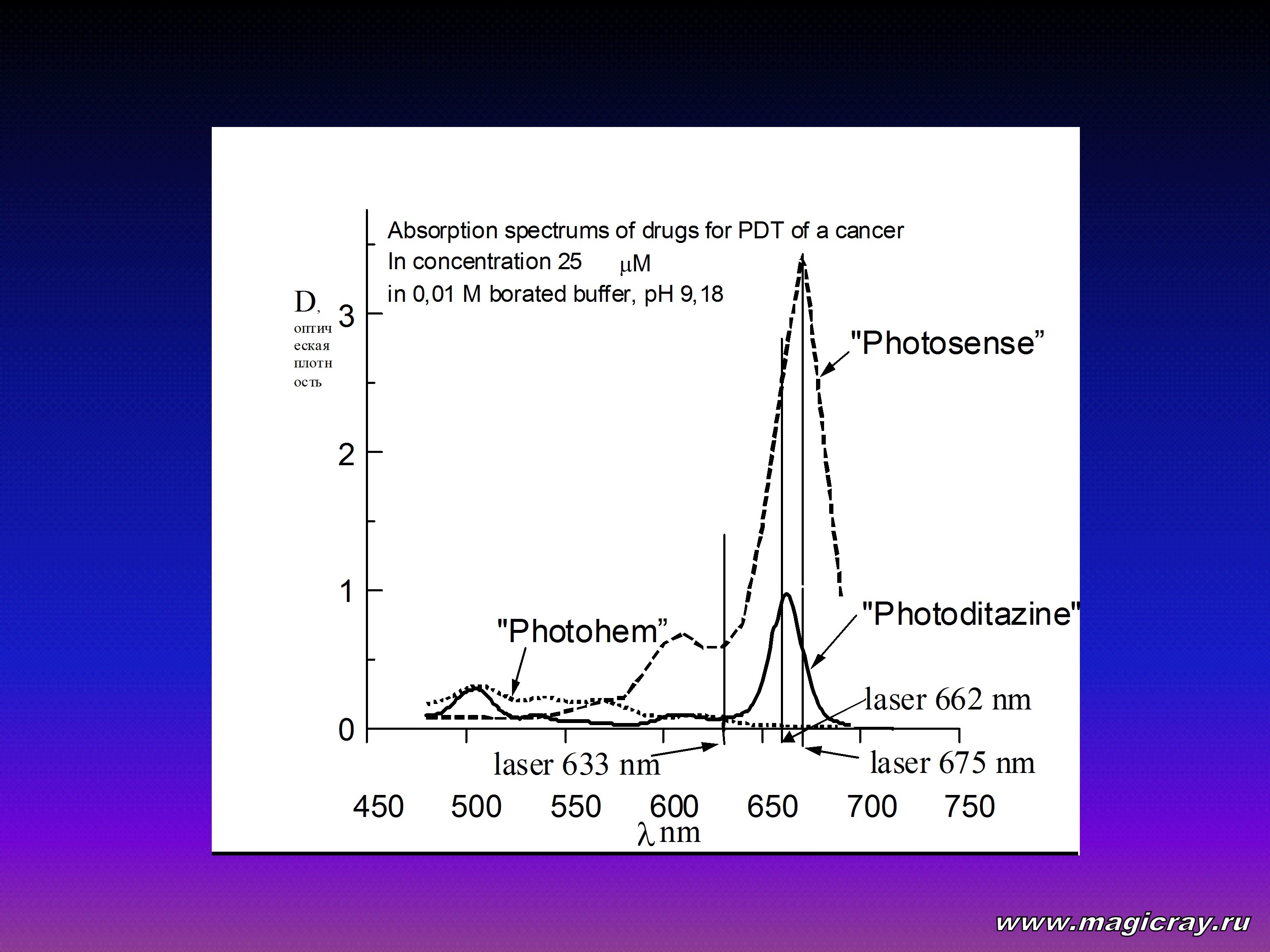
Radachlorin and Photoditazine exhibit a high degree of phototoxicity. This is associated with a high quantum yield of singlet oxygen, which one of the most toxic agents during PDT. Besides that, Radachlorin and Photoditazine show good fluorescence. So, they can be used for fluorescent diagnostics of malignant tumors. The photosensitizers are excited at one of the following wavelengths: 406, 506, 536, 608, or 662 nm. An intense fluorescence is observed at a wavelength of 668 nm. Radachlorin and Photoditazine are highly water-soluble compounds. They also exhibit good stability in storage. When stored in darkness at a temperature of 4 to 8°C, they retain their properties for 18 months.
Chlorin-type tetrapyrrol photosensitizers were put to biological tests. It was found that they absorb eagerly in the far-red and near-infrared bands. They were also found to have an optimum ratio of quantum yields of fluorescence to interconversion. The phototoxicity of these photosensitizers was greater by an order of magnitude than that of many other photosensitizers. These compounds were inactive in darkness. In general, chlorin-type photosensitizers produced a better toxic effect, as compared to both porphyrin oligomeric and sulfonated phthalocyanine compounds. Furthermore, the body eliminated water-soluble chlorin-type compounds much faster. For example, an organism retains Photosense and Photohem for more than 3 months, whereas it eliminates chlorin-type photosensitizers within from 1 till 2 days.
Radachlorin and Photoditazine produced radical changes in the PDT of malignant tumors.
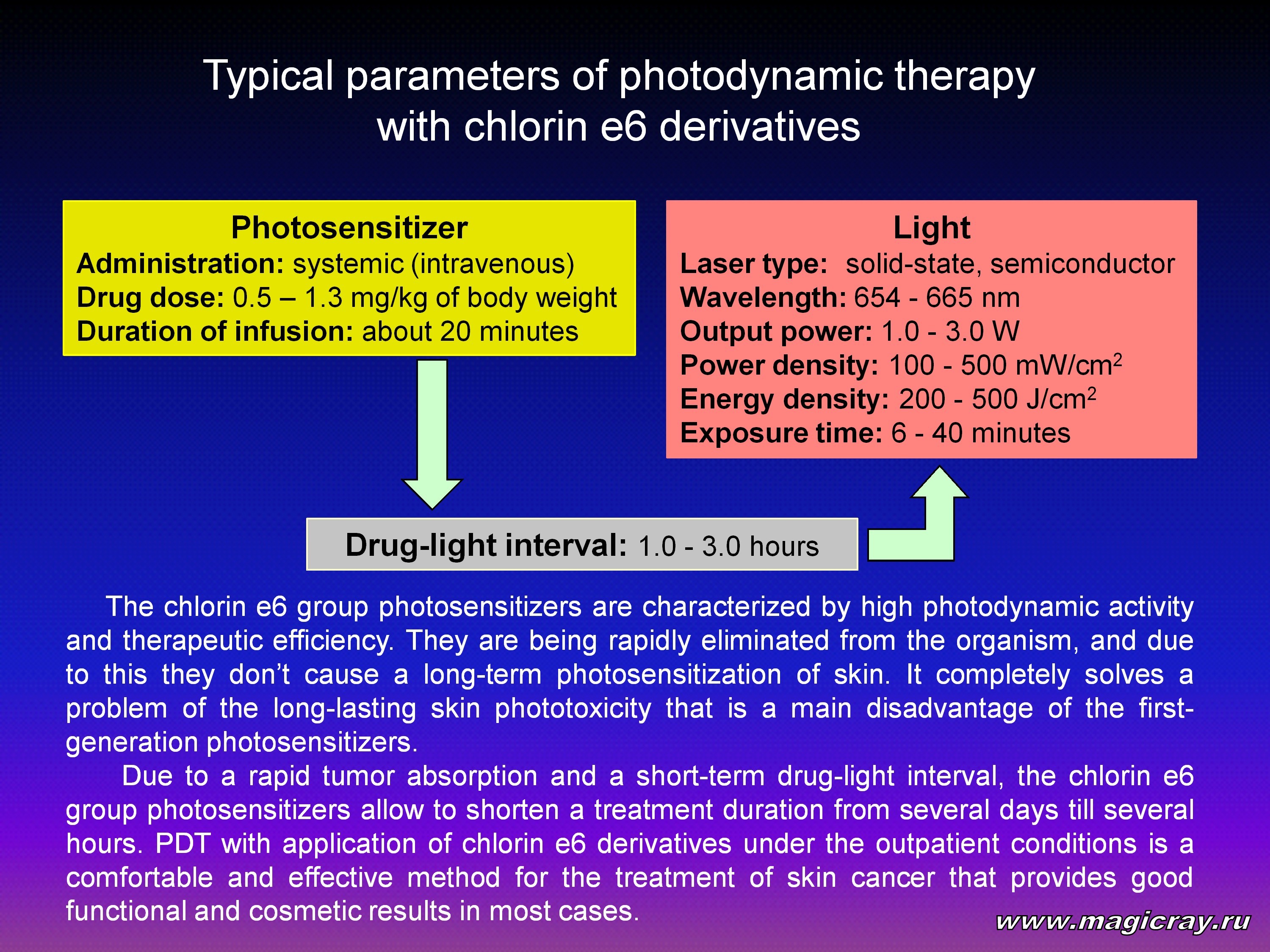
The application of Photofrin II, Photohem, or Photosense relies on a long-term treatment under inpatient conditions, whereas the application of Radachlorin and Photoditazine avoids this stage. Instead, the patient receives a one-day or outpatient treatment. A tumor should be irradiated 2 hours after the photosensitizer injection.





The last several years have seen a considerable progress in antibacterial therapy. However, the problem of infectious diseases ranks high in many medical fields. At present, there are many antibiotic-resistant germs, with Escherichia coli, Staphylococcus aureus, and Streptococci being the most aggressive and resistant bacteria [28, 29]. In the case of a sepsis, staphylococci, fungi, and enterococci are the most resistant germs [30, 31]. The resistance of germs to antibiotics and the need for systemic treatment cause many secondary problems (such as nephro-, hepato-, and neurotoxicities). Among such problems is systemic toxicity of antibacterial compounds. This problem can be considered in terms of a “magic bullet” [32]. The bullet is considered as a microbe-targeting drug. It reacts only with a germ, not with the host. In this context, PDT is such a bullet.
The idea of a “magic bullet” was suggested by Paul Erlikh in the beginning of the 20th century. He hypothesized that the incubation of bacteria with the methylene-blue dye should cause their death at light exposure.
At present, antimicrobial photodynamic therapy (APDT) [32, 33] relies on PDT experience with malignant tumors. Local photosensitizer distribution, local light exposure, fiber-optics involvement, and endoscopic equipment can produce a beneficial clinical effect in some cases.
Current APDT investigations are focused on the intercellular interaction between an activated photosensitizer and infectious agent in vitro.
By now, almost all photosensitizers, optical sources, and infectious agents have been tested.
For example, Z. Malik with co-workers [34] reported a bactericidal effect of PDT on bacteria Staphylococcus aureus, Streptococcus pyigenes, Clostridium perfingens, Escherichia coli, Micoplasma hominis, Gram-negative germs, and yeast fungi.
A. Minnock with co-workers [35] demonstrated that most Gram-negative and Gram-positive bacteria can be effectively photoinactivated by water-soluble phthalocyanines [36]. The methylene-blue dye was found to photoinactivate naked viruses such as the HIV virus [37, 38]. An effective photoinactivation of fungi, including those in the form of spores, was also reported [39].
An effective photoinactivation of cadaver-produced bacteria Helicobacter pylori was reported in 1990. The bacteria were incubated with aluminum sulfonated phthalocyanine and then exposed to 675-nm laser radiation at a dose of 1.5 J/cm2. This brought about an effective destruction of the bacteria. Laser radiation alone at this dose produced no changes in the mucous membrane [40]. In 1992, the photodynamic inactivation of Helicobacter pylori was discussed at the Fifty-Seventh Congress of the American College of Gastroenterology. During the Congress, a comparison was made of photodynamic inactivation and routine eradication. Despite the absence of wide clinical trials, Congress participants showed preference for photodynamic inactivation [41]. The same year, it was reported that cultural bacteria Helicobacter pylori were inactivated by hematoporphyrin derivatives activated by laser radiation at a dose of 50 J/cm2 [42]. In 1997, the European Laser Association published an article by C. E. Milson with co-workers [43]. The researchers reported that, when bacteria Helicobacter pylori had been incubated with the methylene-blue, toluidine-blue, and hematoporphyrin derivative dyes, they were effectively inactivated at doses of 50 and 200 J/cm2. The methylene-blue dye produced the best photoinactivation effect at a dose of 50 J/cm2. It was noted that laser radiation alone at a dose of 50 J/cm2 produced no damaging effect on the mucuous membrane of the stomach [43]. In 1998, C. E. Milson investigated photoinactivation of Helicobacter pylori on animals in vitro. The investigations were made with the toluidine-blue, chloride methylthioninium, hematoporphyrin derivative, and aluminum phthalocyanine dyes. As optical sources, different lasers were used. In the absence of laser radiation, hematoporphyrin and phthalocyanine were moderately bactericide in action.
Proceeding from the general concept of PDT of tumors, scientists are now searching for new ways of increasing the selectivity of photosensitizer accumulation in infectious agents. For example, in order to potentiate the photodynamic effect, the methylene-blue-based PDT was combined with a 1-mA electric current. These experiments were made in vitro on bacteria Escherichia coli. It was found that such a combination increased PDT efficiency [44]. An interesting effect was observed when bacteria were exposed to laser radiation before they were incubated with a photosensitizer. Experiments were made on highly resistant bacteria (such as the bacillus Mycobacterium tuberculosis). It was found that preliminary laser irradiation damaged the bacterial cells. As a result, the bacteria became more liable to APDT attack [45].
Antimicrobial PDT efficiency can be increased by using photosensitizers conjugated with antibodies against bacteria. With this end in view, chlorin e6 was linked to poly-L-lysine. This conjugate was employed in APDT of pathogenic microflora of the oral cavity. The results obtained showed high efficiency of the conjugate in vitro. The conjugate made it possible to increase PDT efficiency and to reduce the light dose down to 15 J/cm2 [46]. S. Devanathan with co-workers [47] conjugated bacterial antibodies with isothiocyanate fluorescent dyes, which were formerly used in fluorescent diagnostics. They demonstrated that such conjugates effectively photoinactivated bacteria Escherichia coli and Salmonella when they were exposed to nonlaser ultraviolet radiation (at wavelengths of 450 to 600 nm).
At present, scientists are trying for increasing the efficiency of antimicrobial therapy based on commercial microbicide drugs. They hypothesized that coherent and noncoherent light of different wavelengths can change the photochemical properties of drugs. To check it, P. Bilski with co-workers [48] combined endogenous vitamin B6 (pyridoxin) with nonlaser radiation at wavelengths of 400 to 550 nm. They demonstrated that such a combination produced a strong toxic effect in vitro on fungi of the genus Cercospora. Fluorquinolone-type antibacterial compounds (such as ofloxacine and lomefloxacine) have been approved for clinical use in many countries. When exposed to ultraviolet radiation, these compounds produce active oxygen forms. This explains skin phototoxicity in the sunlight after administration of these compounds [49].
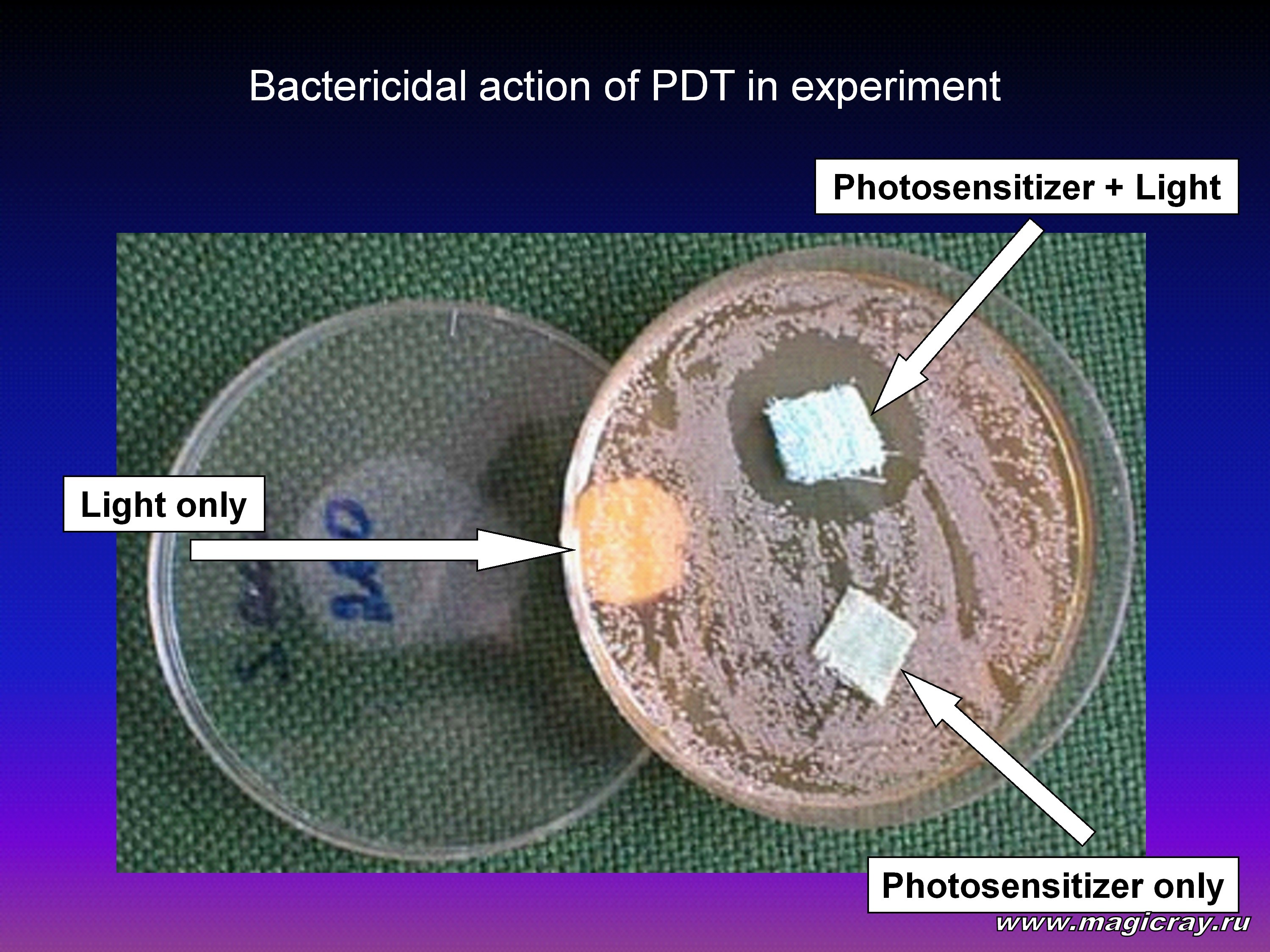
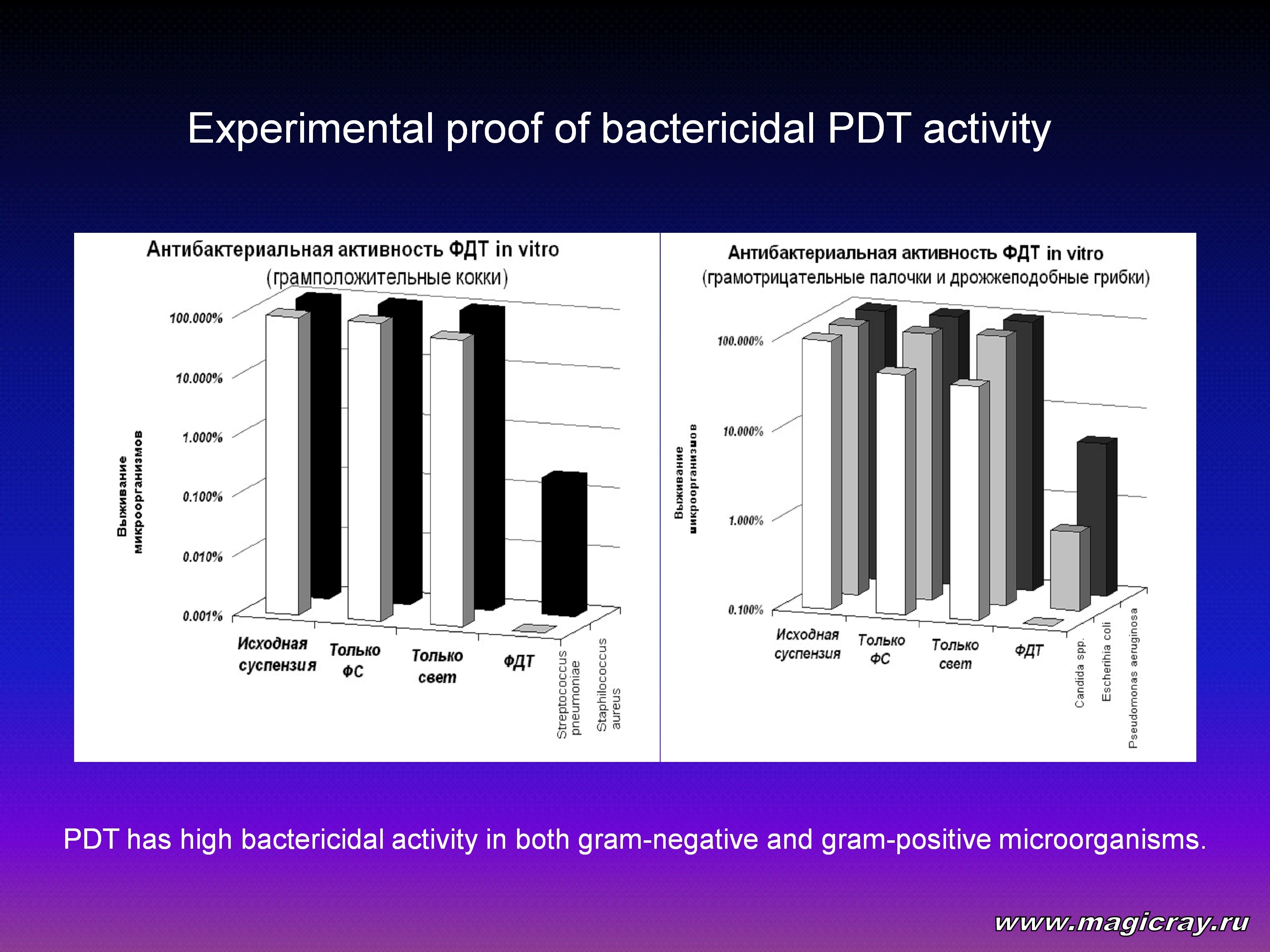
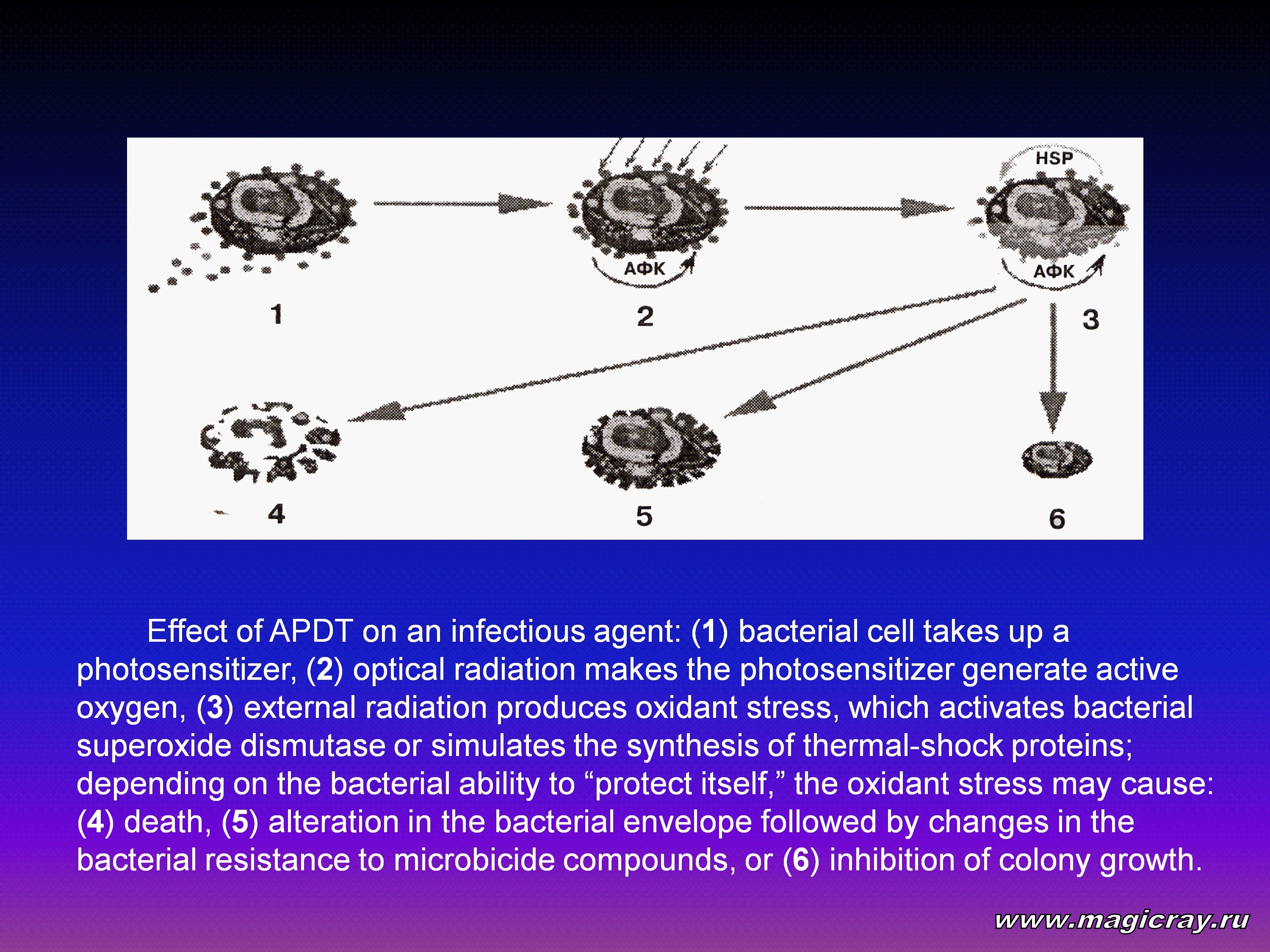
Antimicrobial PDT produces bactericidal and bacteriostatic effects on infectious agents due to the generation of singlet oxygen and peroxide radicals. These substances are generated by extracellular and intracellular photosensitizers. Their action brings about a chain of phototoxic reactions. J. Schneider with co-workers [50] investigated APDT with the methylene-blue dye. Irradiation was performed using a wideband white light source. It produced radiation at wavelengths of 400 to 700 nm. The radiation dose was 10 J/cm2. It was found that such APDT inactivated Qb-bacteriophage RNA in vitro. The RNA was cross-linked to plasmatic proteins. In some cases, oxidant stress inhibited the growth of bacterial cultures in vitro. This effect can also be of use in clinical practice. The bacterial survival after oxidant stress in vitro depends on their superoxide dismutase activity. In the case of Mycobacteria, it also depends on content and activity of thermal-shock proteins. Oxidant stress produces two types of thermal-shock proteins in these bacteria: HSP-70 and HSP-90. It is of interest to subject the bacillus Mycobacterium tuberculosis to APDT in vitro. Investigations were made on viable cultures of Mycobacterium tuberculosis. They were influenced by aluminum sulfonated phthalocyanine (NIOPIK, Russia) and 675-nm laser radiation at a dose of 20 J/cm2. The cultural growth dynamics was assessed by the number and size of colonies. Measurements were made every 10 days for 60 days. The cultures were subjected to photodynamic action on the seventh day. This considerably inhibited the colony growth. Control cultures, which were subjected to the photosensitizer alone or to laser radiation alone, revealed no changes in the colony growth.
Hence, APDT proved to be efficient in the treatment of infectious diseases associated with microbial infections.
In this case, APDT represents an active interaction of active oxygen forms and toxic radicals with bacterial antistress factors. The outcome of this process depends on the generation rate of active oxygen forms, on the activity of antistress proteins, on the action of antioxidant bacterial enzymes, and on many other factors. In some cases, there can be no effect.
Clinical APDT is now in “childhood.” M. Shikowitz with co-workers made a report on PDT of viruses [51]. They employed dihematoporphyrin compounds in PDT of 41 patients with recurrent papillomatosis of the larynx. They regarded papillomatosis as a clinical manifestation of the papillomaviral infection. The patients were injected 3.25 and 4.25 mg of dihematoporphyrin per kg of weight. Endolaryngeal PDT was performed 48 and 72 hours after the injection. To this end, 630-nm laser radiation was employed. The radiation dose was 50 J/cm2. A three-year follow-up study showed a good therapeutic effect, as compared to the control group. A follow-up microscopic examination revealed no papilloma viruses [51].
Other APDT applications are described mainly in Russian papers.
For example, P. Tolstykh with co-workers [52] reported a high APDT efficiency in the treatment of festering wounds in animals. In these experiments, aluminum sulfonated phthalocyanine was applied locally. After that, it was exposed to noncoherent red light. Yu. Alexeev with co-workers was the first to report that hematoporphyrins could treat skin diseases [53]. These researchers investigated the toxicity of porphyrins. These compounds were applied onto the skin and activated by an ultraviolet lamp. Antimicrobial PDT yielded good clinical results in the combined treatment of progressive fibrotic-cavernous tuberculosis. The APDT was carried out using aluminum sulfonated phthalocyanine and intracavernous laser irradiation at a wavelength of 675 nm at a dose of 300 J/cm2. The experiments were headed by Professor A. Ogirenko, Director of the Siberian Center for Laser Medicine (Novosibirsk, Russia). E. Stranadko with co-workers [55] used aluminum sulfonated phthalocyanine in the APDT of chronic suppurative inflammations of soft tissues. They also obtained good clinical results.
Photodynamic therapy produced a therapeutic effect on vasotrophic disorders (such as the chronic venous insufficiency of the lower limbs). This treatment was performed using the Photoditazine photosensitizer and the Crystal 2000 semiconductor laser device (Russia).

This device generates 3-W laser radiation at a wavelength of 662 nm. Clinical trials were conducted at the Hospital Surgery Department of the Samara State Medical University. The experiments were headed by Professors B. Zhukov and S. Musienko.
Photoditazine was applied topically onto an ulcer 2 hours before the PDT session. The photosensitizer was used at a dose of 0.5 ml/cm2. Laser irradiation was performed according to a remote technique with the aid of conventional light-guiding fibers. The PDT parameters (such as the radiation dose, exposure time, and the number of sessions) were selected on an individual basis approach. These parameters depended on the patient’s adaptation characteristics, disease duration, ulcer size, microflora content, bacterial semination, and wound process stage. The results were evaluated from clinical, immunological, microcirculatory, planimetric, and pathophysiological studies. They were also assessed by microbiological, lipid-peroxidation, and morphological examinations (such as cytological and cytobacteriological examinations).

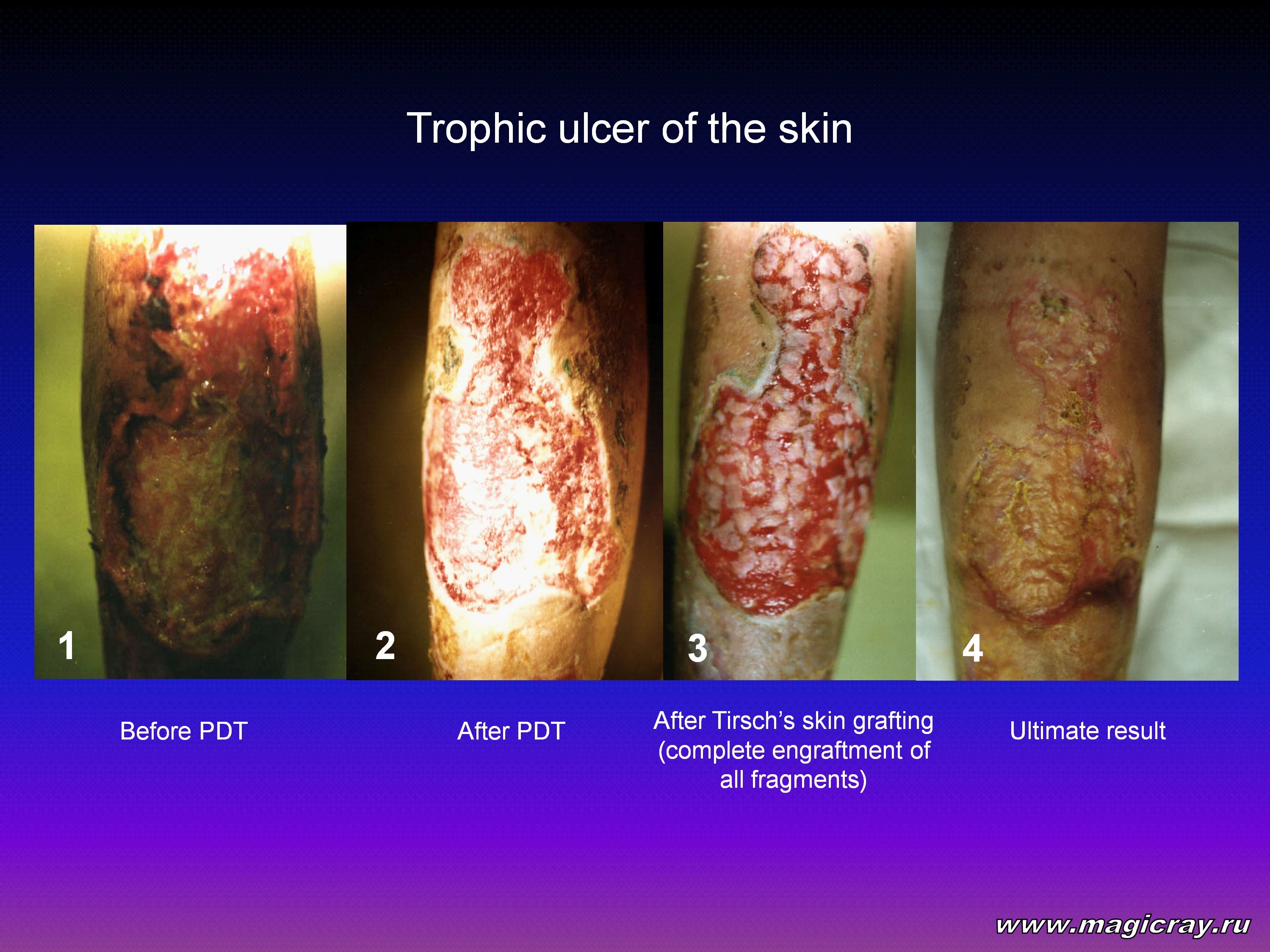
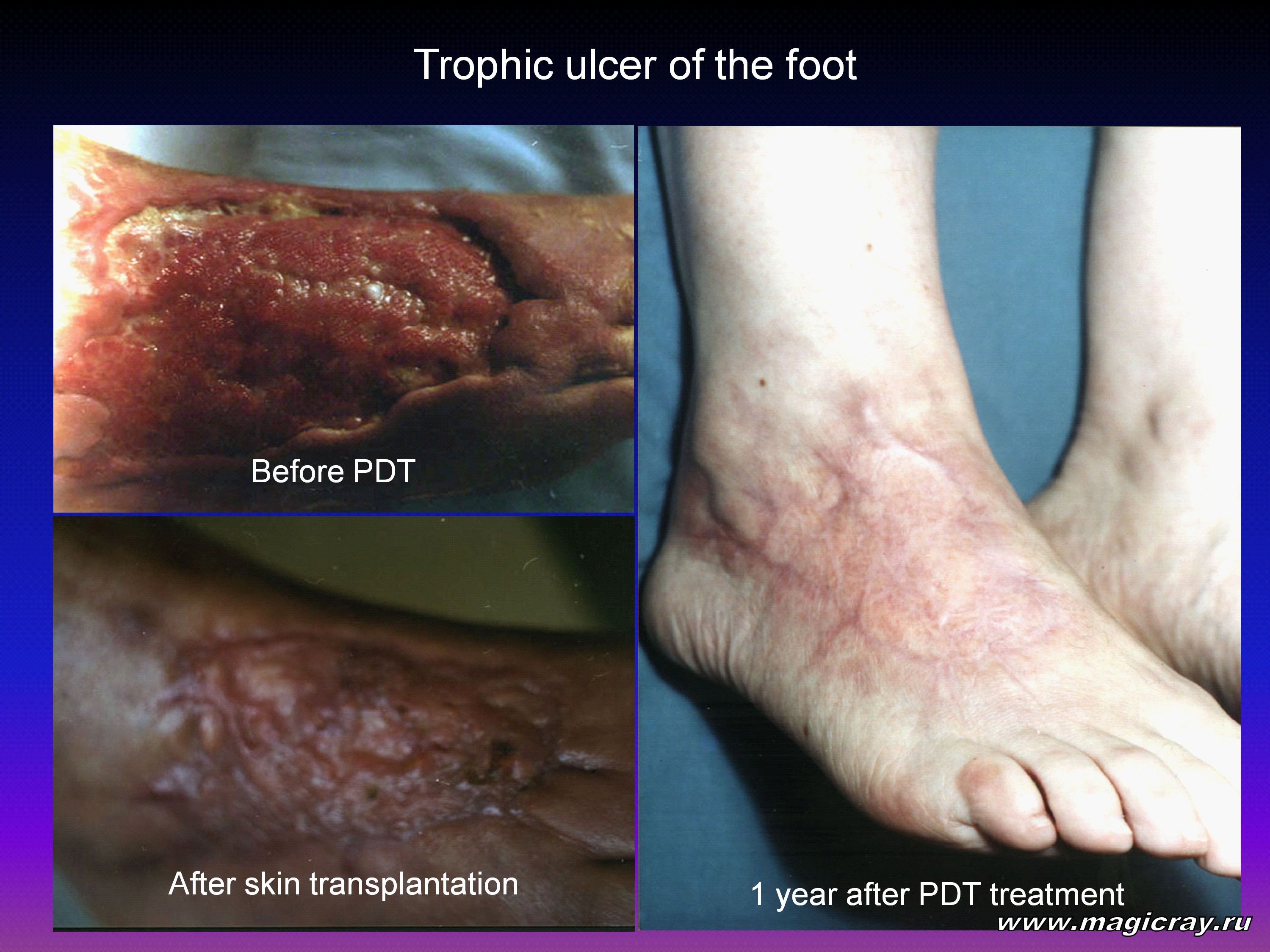
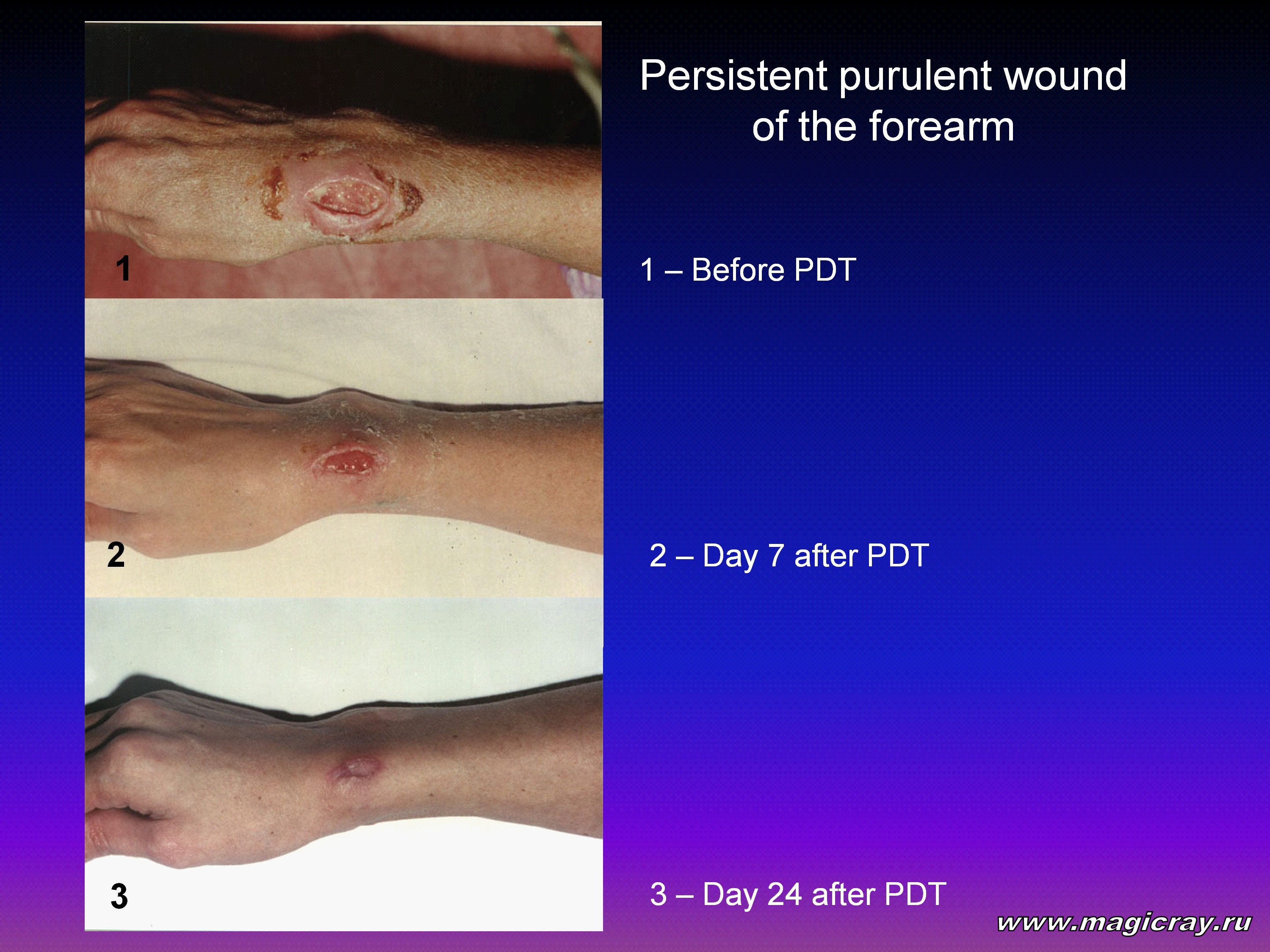
The results obtained were evidence that PDT produced a pronounced antibacterial effect. It also promoted wound necrolysis and stimulated granulation. As a result, PDT shortened the patients’ pretreatment period for dermatoautoplasty by a factor of 1.5 to 2.
Photodynamic therapy produced a clinical effect on duodenal diseases associated with the bacteria Helicobacter pylori. The treatment was performed using aluminum disulfonated phthalocyanine. The experiments were headed by Professor A. Ogirenko at the Siberian Center for Laser Medicine (Novosibirsk, Russia) [56]. Photosense was found to be effective in the APDT of festering ulcers in diabetes-mellitus patients [57]. Antimicrobial PDT seems to have wide application in the future.
Thus, antimicrobial PDT is among the most promising leads in the nonmalignant applications of PDT. It “works” by the principle of the natural antibacterial defense of an organism: it makes use of active oxygen and nitric oxides. It seems promising to combine APDT with traditional antibacterial therapy, physiotherapy, and surgery. Limited APDT application is owing to the lack of comprehensive investigations in this area.
In conclusion, we shall dwell on the advantages of and prospects for PDT of cancer. To begin with, we shall estimate the prevalence of this pathology and the economic damage caused by malignant tumors.
Everybody on Earth feels the negative psychogenic effect of cancer. According to the World Health Organization, in 2001, cancer was first diagnosed in 10 million people, and more than 6 million people died of cancer. Most often, cancer strikes the lung and gastrointestinal tract (stomach cancer, esophagus cancer, colon cancer, and rectum cancer). Lung and gastrointestinal cancer constitutes 47 percent of ten most frequent cancer localizations. They also account for 42 percent of cancer-provoked deaths around the world.
Cancer causes a substantial damage to economy. According to the National Institute of Health, the economic damage of cancer in 2001 reached $180.2 billion in the U.S. alone.
By way of example, consider the economic efficiency of PDT in the treatment of the most frequent forms of cancer. Let us consider accessible tumors. As is known, PDT is most efficient at early stages. Lung and gastrointestinal cancer can rarely be diagnosed at early stages. As a result, despite all of its merits, PDT contributes little to the economy in these cases. The situation changes drastically in the case of skin cancer.
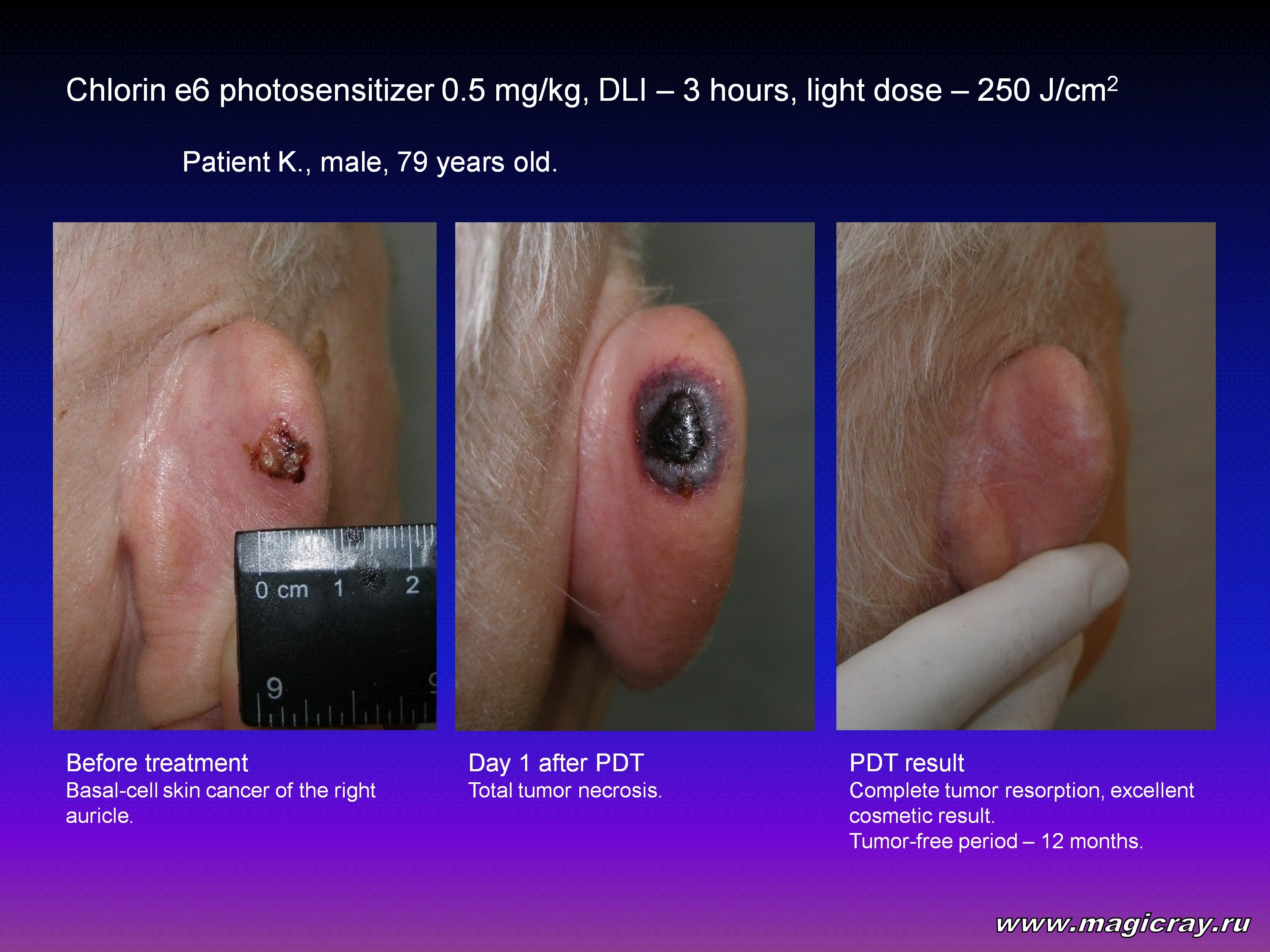
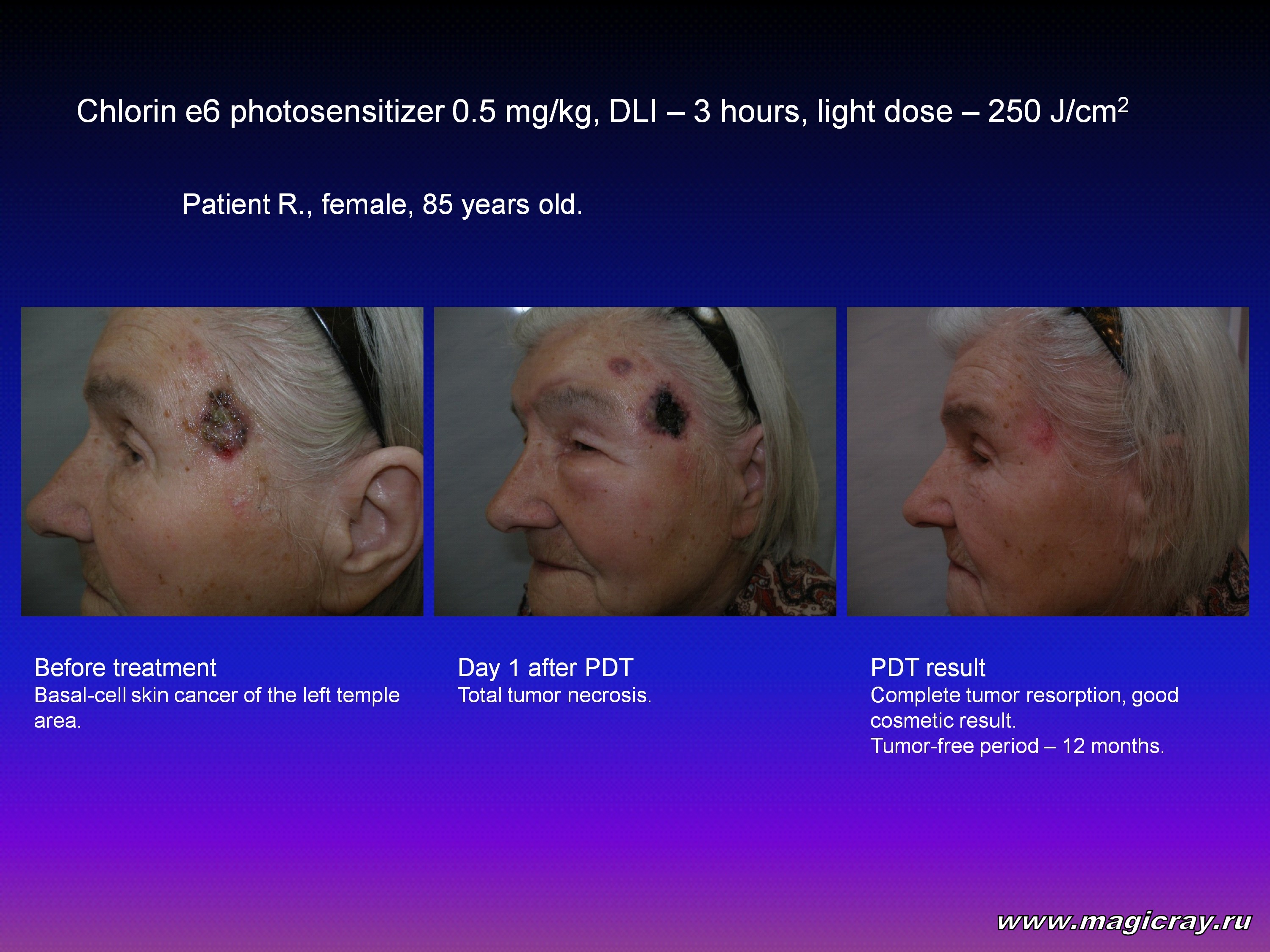
Photodynamic therapy, both in Russia and abroad, is applied in 65 to 70 percent of patients with skin cancer. In this case, PDT yields a 100-percent therapeutic efficiency.
Photodynamic therapy of skin cancer normally requires a single session under outpatient conditions, whereas a routine X-ray therapy lasts for 2 to 3 weeks. In this sense, PDT provides a much better economic efficiency. Photodynamic therapy has a similar effect in the case of other superficial malignant tumors. For example, it goes for recurrences and intradermal metastases of breast cancer, primary tumors and multiple recurrences (up to 60 – 70 percent) of tongue cancer, cancer of oral mucosa, lower-lip cancer, intradermal metastases of melanoma, and other tumors.
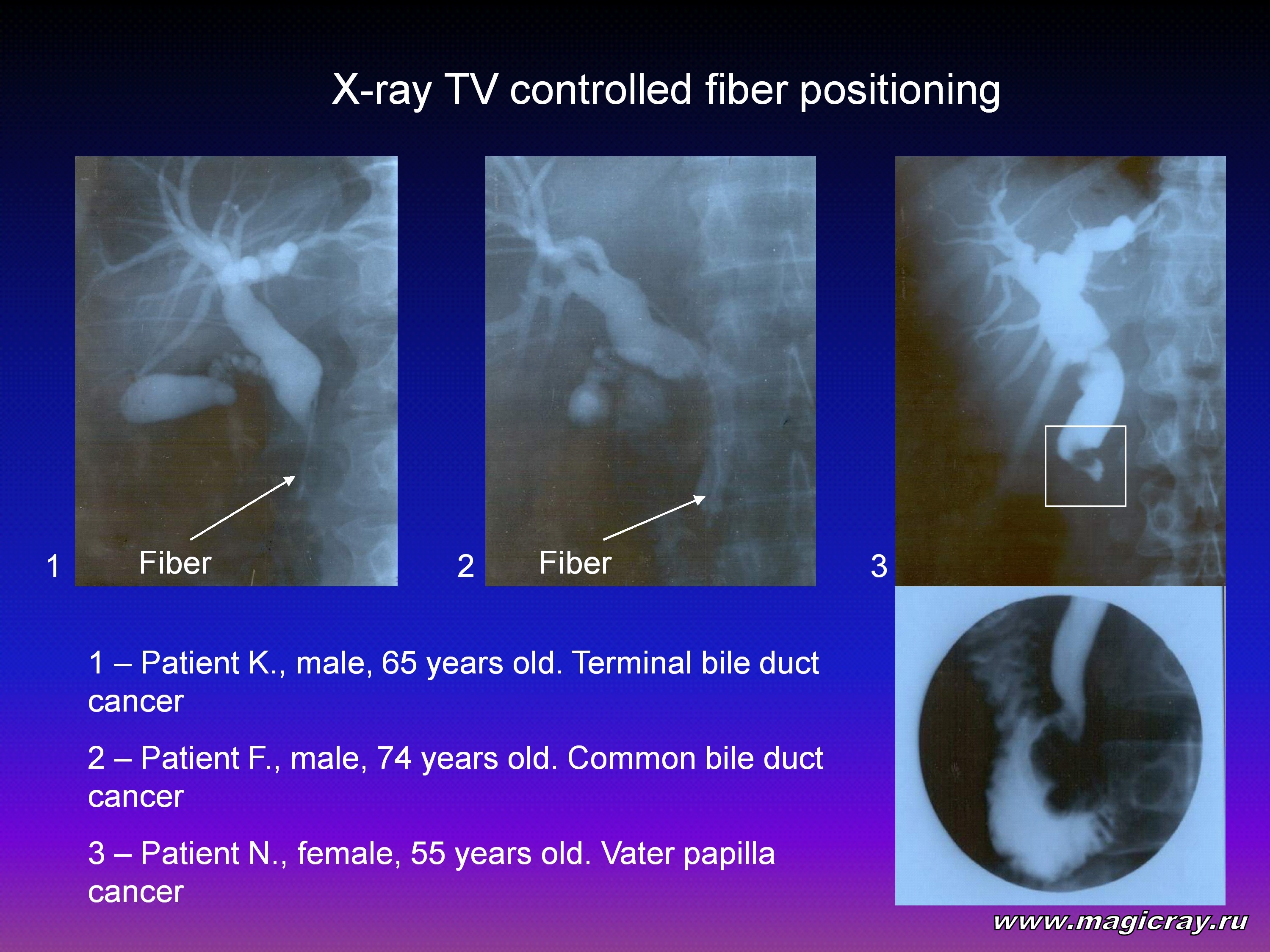
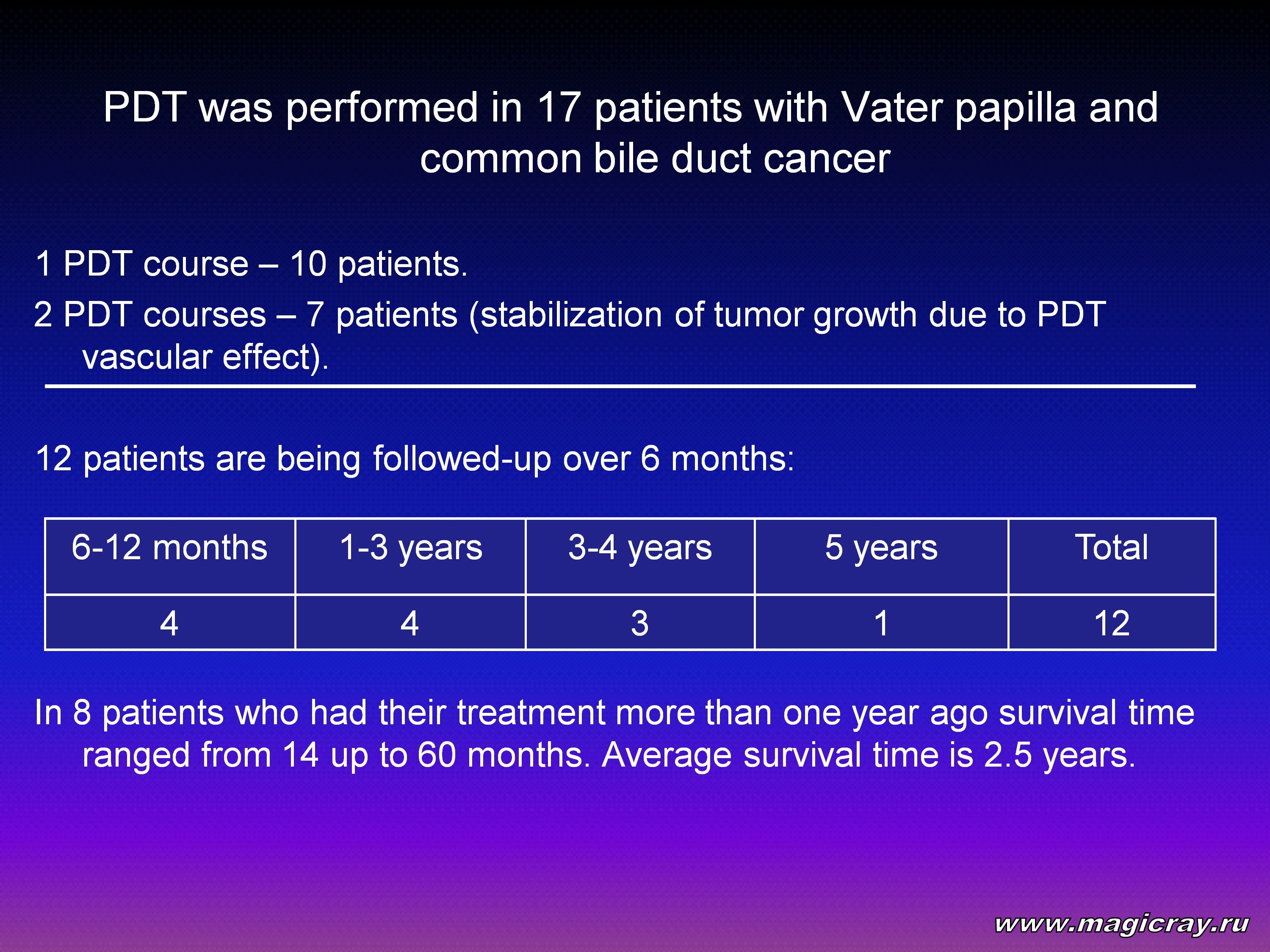
Endoscopic PDT yields good clinical and economic results. In this case, PDT makes it possible to recover lumen of a tumor-obturated esophagus, trachea, and large bronchi. Endoscopic PDT can treat other tumor-stricken internal organs. For example, it can be used in the treatment of hard-to-get-at tumors localized in the pancreaticoduodenal area and common bile duct.


Hence, PDT advantages are as follows:
1. Photodynamic therapy is applied when surgery is contraindicated because of the tumor spread and serious associated diseases. Photodynamic therapy is targeted at tumor cells, and it causes no damage to healthy tissues. Due to this, when PDT has destroyed a tumor, normal cells begin to propagate and fill the organ’s frame. This is of special importance for PDT of thin-walled and tubular organs (such as the stomach, colon, esophagus, trachea, bronchi, and bladder). Photodynamic therapy allows avoiding the organ wall perforation. Thus, the cancer patient with nonresectable tumor has a chance for treatment with use of PDT.
2. Photodynamic therapy produces a targeted effect. A photosensitizer is selectively accumulated in a tumor, and it is rapidly eliminated from healthy tissues that surround the tumor. Due to this, red light selectively damages the tumor, whereas surrounding tissues remain intact.
3. Photodynamic therapy avoids the systemic effect on the human being (in the case of chemotherapy of tumors, this effect does take place). Photodynamic therapy treats an area exposed to light. As a result, the patient is not subjected to an unwanted systemic effect. This makes it possible to prevent the patient from all side effects, typical of chemotherapy (such as nausea, vomiting, stomatitis, loss of hair, and inhibition of hematopoiesis).
4. Photodynamic therapy is cost-effective. For a majority of patients, PDT is a noninvasive or minimally invasive method. It is also a tolerant, local, and inexpensive technique, which can treat a variety of malignant tumors (primary tumors, recurrent tumors, and metastatic tumors).
The Ministry of Health of Russia analyzed the results of PDT application in Moscow Medical Centers. Photodynamic therapy was employed to treat malignant tumors of the skin, breast, oral mucosa, tongue, lower lip, larynx, lung, esophugus, stomach, bladder, and rectum. From 1992 to 2001, PDT was used to treat more than 1,600 tumors in 408 patients. Most of the patients had been treated earlier with routine methods (such as surgery, radiotherapy, and combined treatment). Some of the patients had not been treated earlier owing to serious age-related and associated diseases. The rest of the patients received palliative PDT. They had extended obturating tumors of the esophagus, trachea, colon, large bronchi, and cardia. Photodynamic therapy was performed to recanalize stenosed organs and to improve the quality of life. Follow-up studies had been made for 2 months to 9 years. Photodynamic therapy produced a beneficial effect in 94.4 percent of the patients. Of these, 56.2 percent showed a complete tumor resorption, and 38.2 percent showed a partial tumor resorption.
Photodynamic therapy is an advanced therapeutic technique, which is employed in Russia with success. At present, new photosensitizers and optical sources are being developed for PDT and fluorescent diagnostics. Photodynamic therapy is a promising, cutting-edge, and cost-effective method for treatment of malignant and nonmalignant diseases. To disseminate information about this technique, PDT-oriented workshops and schools should be arranged for physicians.
References
- El-Mofy A.M. Vitiligo and Psoralens. – Oxford: Pergamon Press, 1968. – 147 p.
- Wyss P. History of Photomedicine // Wyss P., Tadir Y., Tromberg B.J., Haller U. (eds): Photomedicine in Gynecology and Reproduction. – Basel: Karger, 2000. – P. 4-11.
- Fahmy I.R., Abu-Shady H.: Ammi majus linn: The isolation and properties of ammoidin, ammidin and majudin, and their effect in the treatment of leukoderma // J. Pharm. Pharmacol. – 1948. – Vol. 21. – P. 499-503.
- Abels C., Goetz A.E. A clinical protocol for photodynamic therapy // H.Honigsmann, G.Jori, A.R.Young (eds): The Fundamental Bases of Phototherapy / OEMF spa – Milano, 1996. P. 265-284.
- Rasmussen D.S., Ward G.E., Figge F.H.J. Fluorescence of human lymphatic and cancer tissues following high doses of intravenous hematoporphyrin // Cancer. – 1955. – Vol. 1. – P. 78-81.
- Tappeiner H., Jesionek H. Therapeutische Versuche mit fluoreszierenden Stoffen // Munch. Med. Wschr. – 1903. – Vol. 50. – P. 2042-2044.
- Jesionek H., Tappeiner H. Zur Behandlung der Hautcarcinome mit fluoreszierenden Stoffen // Dtsch. Arch. Klin. Med. – 1905. – Vol. 82. – P. 223-226.
- Tappeiner H., Jodlbauer A. Uber die Wirkung der photodynamischen (fluoreszierenden) Stoffen auf Protozoen und Enzyme // Dtsch. Arch. Klin. Med. – 1904. – Vol. 80. – P. 427-437.
- Hausmann W.H. Die sensibilisierende Wirkung des Hamatoporphyrins // Biochem Z. – 1910. – Vol. 30. – P. 276-316.
- Hausmann W.H. Die sensibilisierende Wirkung tierischer Farbstoffe und ihre physiologische Bedeutung // Wien. Klin. Wochenschr. – 1908. – Vol. 21. – P. 1527-1529.
- Meyer-Betz F. Untersuchung uber die biologische (photodynamische) Wirkung des Hamatoporphyrins und anderer Derivate des Blut- und Gallenfarbstoffs // Dtsch. Arch. Klin. Med. – 1913. – Vol. 112. – P. 476-503.
- Policard A. Etudes sur les aspects offerts par des tumeurs experimentales examines a la lumiere de Wood // CR Soc. Biol. – 1924. – Vol. 91. – P. 1423-1424.
- Auler H., Banzer G. Untersuchung uber die Rolle der Porphyrine bei geschwulstkranken Menschen und Tieren // Z. Krebsforsch. – 1942. – Bd. 53. – S. 65-68.
- Figge F.H.J., Weiland G.S., Manganiello O.J. Cancer detection and therapy. Affinity of neoplastic, embryonic, and traumatized tissues for porphyrins and metalloporphyrins // Proc. Soc. Exp. Biol. Med. – 1948. – Vol. 68. – P. 640-641.
- Schwartz S., Absolon K., Vermund H. Some relationships of porphyrins, X-rays and tumors // Bull. Minn. Univ. School Med. – 1955. – Vol. 27. – P. 7-13.
- Lipson R.L., Baldes E.J., Olsen A.M. The use of a derivative of hematoporphyrin in tumor detection // J. Nat. Cancer Inst. 1961. – Vol. 26. P. 1-8.
- Gregorie H.B., Horger E.O., Ward J.L. et al.Hematoporphyrin-derivative fluorescence in malignant neoplasms // Ann. Surg. – 1968. – Vol. 167. – P. 820-828.
- Lipson R.L., Gray M.J., Baldes E.J. Hematoporphyrin derivative for detection and management of cancer / Proc. 9-th International Cancer Congress. – Tokyo, Japan, 1966. – 393 p.
- Diamond I., McDonagh A.F., Wilson C.B. Photodynamic therapy of malignant tumors // Lancet. – 1972. – P. 1175-1177.
- Kelly J.F., Snell M.E. Hematoporphyrin derivative: a possible aid in the diagnosis and therapy of carcinoma of the bladder // J. Urol. – 1976. – Vol. 115. – P. 150-151.
- Dougherty T.J. Studies on the structure of porphyrins contained in Photofrin II // Photochem. Photobiol. – 1987. – Vol. 46 (5). – P. 569.
- Dougherty T.J. Photodynamic therapy – new approaches // Seminars in Surgical Oncology. – 1989. – Vol. 5. – P. 6-16.
- Hayata Y., Kato H., Konaka C. et al. Hematoporphyrin derivative and laser photoradiation in the treatment of lung cancer // Chest. – 1982. – Vol. 81. – P. 269-277.
- Dougherty T.J., Thoma R.E., Boyle D., Weishaupt K.R. Photoradiation therapy for the treatment of malignant tumors: Role of the laser // Laser in Photomedicine and Photobiology R. Pratesi, C.A. Sacchi (eds). – New-York: Springer, 1980. – P. 67-75.
- Kessel D., Thompson P., Musselman B., Chang C.K. Probing the structure of the tumor-localizing derivative of hematoporphyrin by reductive cleavage with LIAIH4 // Photochem. Photobiol. – 1987. – Vol. 46 (5). – P. 563.
- Dougherty T.J., Kaufman J.E., Goldfarb A. Photoradiation therapy for the treatment of malignant tumors // Can. Res. – 1978. – Vol. 38. – P. 2628-2635.
- Bugelski P.J., Porter C.W., Dougherty T.J. Autoradiographic distribution of hematoporphyrin derivative in normal and tumor tissue of the mouse // Cancer Res. – 1981. – Vol. 41. – P. 4606-4612.
- Amyles S. // JAMA. – 2001. – Vol. 285, № 18. – P. 2317-2318.
- Stephenson J. // JAMA. – 2001. – Vol. 285, № 18. – P. 2318-2319.
- Гельфонд Б.Р. // Инфекции и антимикробная терапия. – 2001. – Т. 3, № 3. – С. 3-4.
- Яковлев С.В. // Инфекции и антимикробная терапия. – 2001. – Т. 3, № 3. – С. 6-7.
- Wainwright M. // J. Antimicrob. Chemother. – 1998. – Vol. 42. – P. 13-28.
- Zeina B., Greeman J., Purcell W., Das B. // Brit. J. Derm. – 2001. - № 144 (2). – P. 274-278.
- Malik Z., Hanania J., Nitzan Y. // J. Photochem. Photobiol. B: Biology. – 1990. – Vol. 5. – P. 281-293.
- Minnock A., Vernon D.I. et al. // J. Photochem. Photobiol. B: Biology. – 1996. – № 32 (3). – P. 159-164.
- Minnock A., Vernon D., Schofield J. et al. // Antimicrob. Agents Chemother. – 2000. – Vol. 44, № 3. – P. 522-527.
- Mohr H., Lambrecht B., Selz A. // Immunological investigation. – 1995. – Vol. 24. – P. 73-83.
- Bachmann B., Knuver-Hopf J., Lambrecht B. // J. Med. Virology. – 1995. Vol. 47. – P. 172-178.
- Jackson Z., Meghji S., McRobert A.M. // 1999. – Vol. 14. – Iss. 2. – P. 150-157.
- Bedvell J. et al. // The Lancet. – 1990. – Vol. 335, № 8700. – P. 1287.
- Wolfsen H. et al. 57-th Annual Meeting American College of Gastroenterology // Miami Beach, 1992.
- Wolfsen H. et al. // Photodynamic therapy and biomedical lasers. Ed.: P. Spinelli. – M/Dal Fante dc Marchellini. – Amsterdam, 1992. – P. 281-285.
- Milson C. et al. // Ann. Univ. College. – London: Medical School, 1998. – On-Line.
- Capella M., Menezec S. // Int. J. Radiat. Biol. – 1992. – Vol. 62 (3). – P. 321-326.
- Волкова А., Лощенов В., Ершова Е. и др. Лазерные и информационные технологии в медицине XXI века / Материалы международной конференции. СПб., 2001. – С. 414.
- Soukos N. et al. // Antimicrob. Agents Chemother. – 1998. – Vol. 42, № 10. – P. 2592-2601.
- Devanathan S., Dahl T., Midden W. et al. // Proc. Nat. Acad. Sci. USA. – 1990. – Vol. 87. – P. 2980-2984.
- Bilski P., Ehrenshaft M., Daub M. et al. // Photochemistry and Photobiology. – 2000. – Vol. 71 (2). – P. 129-134.
- Ferguson J. // Photochem. Photobiol. – 1995. – Vol. 62. – P. 954-958.
- Schneider J., Quentin P., Floyd R. // Photochem. Photobiol. – 1999. – Vol. 70 (6). – P. 902-909.
- Shikowitz M., Abramson A., Freeman A. et al. // Laryngoscope. – 1998. – Vol. 108 (7). – P. 962-967.
- Толстых П., Корабоев У., Шехтер А. и др. // Лазерная медицина. – 2001. - № 5 (2). – С. 8-13.
- Алексеев Ю., Гладких С., Иванова И. и др. // Материалы 2-го Всеросс. симпозиума «Фотодинамическая терапия злокачественных новообразований». – М., 1997. - С. 142-144.
- Огиренко А., Денисов А., Васильев Н. и др. // Материалы 3-го Всеросс. симпозиума «Фотодинамическая терапия». – М., 1999. - С. 53-54.
- Странадко Е., Толстых П., Корабоев У. // Материалы 3-го Всеросс. симпозиума «Фотодинамическая терапия». – М., 1999. - С. 83-91.
- Васильев Н.Е. // Лазерная медицина. – 1999. – Т. 3 (3-4). – С. 16-20.
- Толстых П., Корабоев У., Дуванский В. и др. // Материалы междунар. конф. «Лазерные и информационные технологии в медицине XXI века». – СПб., 2001. – С. 449-450.
|
