3. Causes of Cancer Development
The “Magic Ray” Moscow Center of Laser Medicine, Moscow, Russia
Introduction
I worked as an oncologist before medicine entered the photodynamic therapy (PDT) epoch. Today, I may state: “Of course, oncologists have made a considerable progress in tumor destruction. They have surgery, chemotherapy, radiotherapy, and combined therapeutic techniques. However, statistics shows that oncologists are doing the Sisyphean toil.”
The world statistics demonstrates that malignant tumors rank second among the causes of death. Every 16 minutes, there on Earth appears a man with cancer. Therefore, oncologists have to destroy the tumor, not the patient. This should be the main objective of all oncologic approaches.
I have seen cancer patients suffering greatly. Such patients included my relatives too. Sympathy for these patients motivated us to develop a technique for PDT pretreatment. To gain an insight into this technique, we need to consider the causes of cancer.
Modern Science about Carcinogenic Mechanisms
The last 10 years have seen drastic changes in the scientific concept of cancer development. Presently, there are at least three fundamental mechanisms of cancer development.
Mechanism One. It is based on oncogenes, which are normally responsible for cell division and growth. Radiation or chemicals may cause mutations in them. For example, cigarette smoke may provoke such mutations. A mutated oncogene stimulates uncontrolled division of cells. As a result, cells begin to divide continuously, forming a tumor. Earlier, it was thought that cancer resulted from a virus. For example, American scientist Peyton Rous discovered a tumor virus in chickens. It took 55 years for Rous’ discovery to advance to its dominant place in cancer research. In 1966, Rous was awarded the Nobel Prize in medicine. However, in 1976, it was established that viruses by itself did not cause cancer. They acted as an oncogene transmitter. Two Americans Michael Bishop and Harold Varmus from California proved it experimentally. In 1989, they were also awarded the Nobel Prize in medicine. However, oncogenes were not the only causes of cancer.
Mechanism Two. As turned out, it was not enough to simply “turn on” the oncogenes. It was also necessary to “turn off” protector genes. They protected cells from oncogene-associated malignancy. In 1992, it was confirmed by experiments on mice.
Mechanism Three. It is based on destabilizer gene activation and immune disorders.
Recently, there was a metastasis gene discovered. It disallows cells to invade the vascular wall. This gene is spread to other sites via the bloodstream. Some time later, researchers detected a stabilizer gene, which governs the mutation rate of other genes.
So, the number of cancer development mechanisms is increasing. Cancer can arise from activation of some particular genes. Each patient may have his or her own genes. Furthermore, there can be genes unknown to modern science.
In addition to the aforementioned fundamental mechanisms, cancer development may involve other factors. They are related to the person’s mode of life, internal state, and outdoor environment.
A growing rate of malignant diseases is associated with changes in our habits, ways of living, and spiritual life. For example, self-actualization governs our emotional and spiritual states. Self-dissatisfaction and repeated stresses can affect enzymic, hormonal, and metabolic systems. In turn, this affects the immune system. As a result, a group of cells may run out of control. The cells begin to live their own way: they exhibit abnormal and uncontrolled division, which forms a malignant tumor. This process lasts for many years and manifests itself at the final phase. Precancer may lurk in the body for years and decades. It may take 10 to 20 years for a single cancer cell to grow into a 2-millimeter tumor. Rapidly growing tumors develop faster: for 6 years. Physicians can detect a tumor of a size of 2 to 3 millimeters. The tumor reaches a size of about 10 mm for the next 2 to 6 years. Physicians can detect such a tumor by palpation (late detection). Note, the sooner the tumor detection, the better for the patient.
Radical operation, radiotherapy, or chemotherapy cannot treat a person’s predisposition to cancer. Hence, these therapies cannot prevent the patient from tumor relapses. Conversely, they inhibit the patient’s immune system and thus promote recurrences. To cancel side effects, one needs to combine present-day therapies with immune and spiritual strengthening. There are several cases of a person’s self-healing. For example, a patient underwent a surgery, which caused spread tumor metastases. As a result, the cancer became inoperable. When sutures healed over, the patient was discharged on symptomatic treatment. In this case, physicians betrayed the patient. They had to do it owing to the modern medicine feebleness. However, some time later, the patient recovered from the disease due to self-healing. If needed, anyone can do it. To this end, the ego should rebel against the weak will. This helps the person to get over the disease. A profound psychogenic stress changes the person’s mind, makes him revalue cultural wealth, and inspires a desire to achieve lofty aims. These may rescue a patient from a fatal disease.
Hence, complex actions can overcome cancer. These actions should stimulate the patient’s defense mechanisms. Both the physician and the patient have to fight the disease. The patient should take offensive actions, not defensive. Lively faith in own strength works wonder!
People are known to reveal genetic predisposition to tumors. Such predisposition strikes particular organs (such as the lungs, stomach, and liver), not the entire body. There are some cases where a defective gene passed from generation to generation, and then it took away many relatives: they all died of cancer that had affected the same organ. However, it was discovered quite recently that genetic predisposition to cancer becomes apparent at the early stage of organism development. This predisposition manifests itself by disorders in the intercellular interaction. For example, the bonding force of healthy epithelium was found to exceed that of cancerous epithelium-on the average-by an order of magnitude. This made it possible to relate genetic predisposition to cancer to the mechanical properties of biological tissues. This finding is of great practical importance. It enables us not only to predict cancer at an early age but also to increase tolerance to it. This can be done by increasing the bonding force of some organ-specific cells.
Immunity and Tumors
Tumor progression depends on hormonal regulation, immune reactions, as well as on many genetic causes (we know only some of them). However, we should focus our attention on the immune state. A strong immune system kills tumor cells, whereas an inhibited immune system may initiate cancer development. However, as soon as the immune system gathers strength, the tumor progression stops and degrades. Stimulating the immune system acts indirectly on the tumor. It was established that clinical signs of malignant tumors followed immune-system failures. In this case, immune cells become unable to devour tumor cells that continuously appear in the body. Treatment with medicinal herbs, bee products, and other folk remedies is aimed at stimulating immune responses. Modern medicine is actively searching for immune-stimulating methods. The development of anticancer vaccines seems to yield encouraging results. For example, M.Mitchel from South California was the first to test successfully a cancer-specific vaccine. The vaccine was tested in 13 women with fatal breast cancer. After the treatment, the tumor shrank and resolved in 8 women. The vaccine appeared to be less effective in melanoma treatment. However, my experience in PDT application to eye melanoma has demonstrated some encouraging results.
Among factors inhibiting the immune system and thus favoring cancer is an excess use of hormones and tranquilizers. Their application produces a negative effect on the immune system. For example, synthetic sedatives can effectively mitigate stress, anxiety, and worry. However, they pollute the internal environment of the human body. The trace concentrations of these compounds can circulate in the bloodstream for weeks and months. Furthermore, these compounds suppress the natural ability of human subjects to overcome stress. A regular intake of tranquilizers also deranges some specific antistress mechanisms.
It was also hypothesized that cancer may arise from the absence of inflammatory processes, rapid suppression of inflammatory reactions with antipyretic remedies, and multiyear decrease in the bodily temperature (normally, it ranges from 36 to 36.9°C). According to this hypothesis, one should not quickly take antipyretic remedies to bring the temperature down. It is better to let the organism by itself fight a slight cold or influenza. Overcoming the disease strengthens the immune system, which is the best protection from cancer.
Alternative Present-Day Theories of Carcinogenic Mechanisms
Doctor Clark from the U.S. has advanced a theory of toxic cell damaging by ecological crises. The scientist proceeded from the fact that every living cell of a human body is attacked by 100,000 adverse environmental factors (such as heavy metal salts, pesticides, and other numerous carcinogens).
Doctor Tamara Svishcheva from Russia resolves another theory of cancer, AIDS, diabetes, and vascular pathology. In her book “Panacea for Cancer, Infarction, and AIDS”, which was published in 2001, she justified the parasitic nature of cancer.
Stained slides of peripheral and venous blood of human beings were examined using optical microscopy. Their correct interpretation revealed pathological changes in the blood cells. It also showed biological structures that were responsible for these changes (such as trichomonads, thrombocytes, streptococci, staphylococci, and fungi).
Doctor Tamara Svishcheva compiled the “Atlas of Human Blood Cells and Parasites”. It displays the histological features of Trichomonas hominis, Trichomonas vaginalis, Trichomonas tenax, as well as tumor cells of man and animals. Hematologists often mistake Trichomonas hominis (which live in blood) for blood and marrow cells. The author conducted experiments in several world-renowned institutes of Russia. The results obtained showed the morphological identity of trichomonads at cellular, molecular, and genetic levels. It was concluded that elimination of trichomonads from human blood and organs would avoid tumor and thrombocyte formation. As a result, this would avoid the development of cancer, infarction, and AIDS.
The aforementioned book is addressed to a broad range of readers, who are interested in their health.
Forgotten Notions of Trichomonas – Blood Parasites
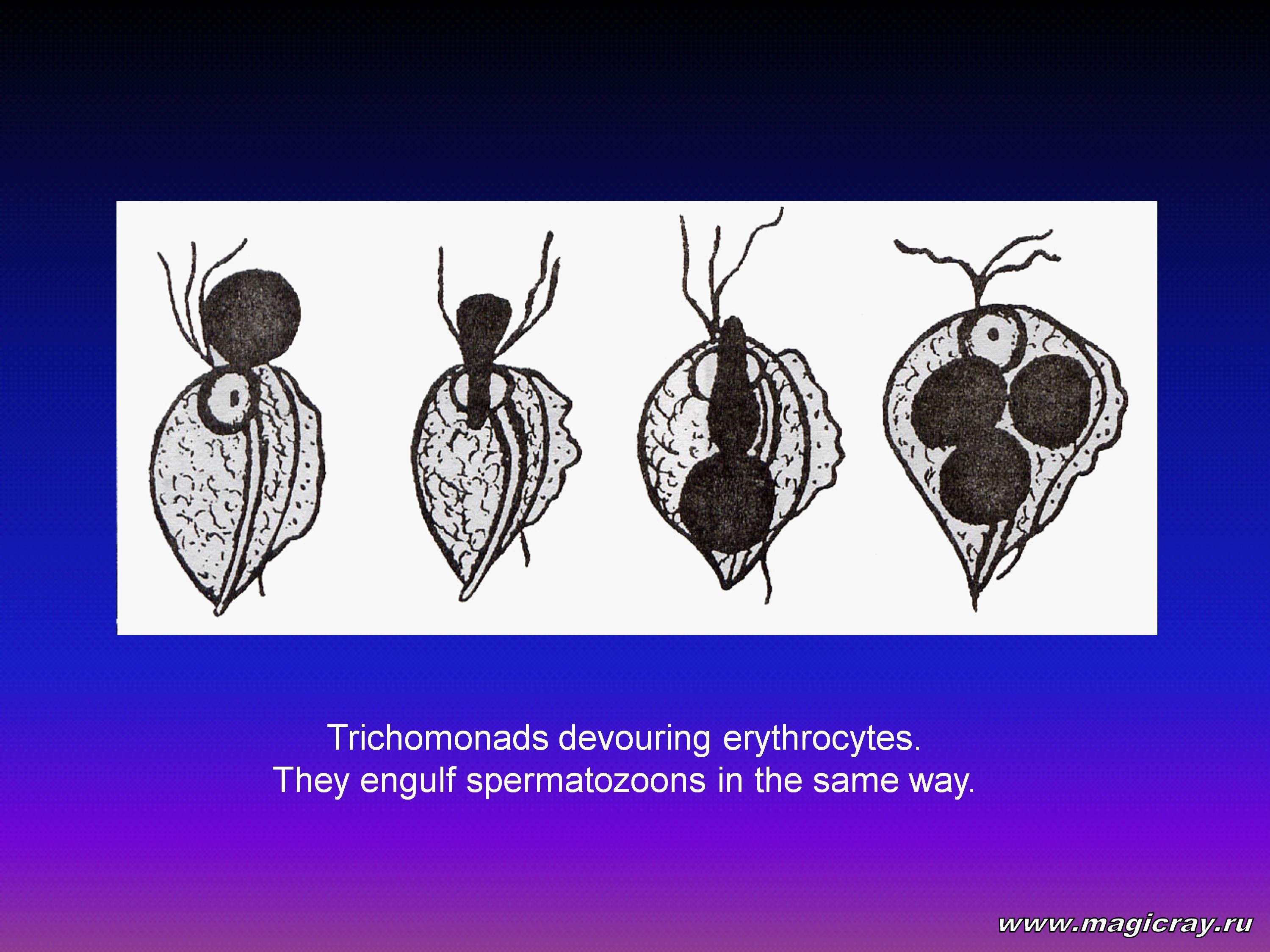
In the postwar years, prominent Academician of the U.S.S.R. Medical Academy of Sciences, parasitologist E.Pavlovsky detected trichomonads in many venous-blood samples taken from diseased people. E.Pavlovsky, E.Visir’, and other researchers continued laboratory investigations on these parasites. As a result, they described trichomonad behavior in blood. In his “Textbook on General Parasitology” E.Pavlovsky presented the photographs of trichomonads, which sequentially engulfed up to three erythrocytes.
This provided evidence that, although trichomonads were cavity parasites, they were able to invade the body. When a trichomonad invades blood, it acts as a predator that devours red blood cells. A trichomonad can come into blood from genitals. In this case, it carries – in its vacuole – phagocytosed, but undigested, sexually transmitted germs. Most often, these germs are chlamydias, which are something in-between viruses and bacteria. Their development passes two cycles: intracellular and extracellular.
When a trichomonad engulfs chlamydia, the latter turns into a parasite. In this case, chlamidya releases poisonous enzymes. The host defends itself and isolates the aggressor. To this end, it forms a vacuole - a cavity in the cell cytoplasm filled with cellular juice. The juice consists mainly of lipids - fatty substances. On the one hand, the lipids neutralize chlamydial toxins. On the other hand, they serve as food for the chlamydia and its offspring. Hence, in order to neutralize its internal parasites, the trichomonad becomes an aggressive predator. To feed not only itself but also the chlamydia, the trichomonad constantly needs to devour blood cells and microbes.
A similar situation happens when a trichomonad is invaded by other parasites (such as the oncogenic measles virus, herpes simplex virus, and epidemic parotitis virus). The last virus causes an acute viral disease that mainly affects parotid glands. I described this process in one of my books, in the chapter “Victims of Multiple Sclerosis”. In that book, trichomonads were disturbed by intrinsic parasites. To neutralize these parasites, trichomonads filled themselves with cholesterol. To this end, they devoured the myelin sheath of nerve trunks. Because of this, the parasites caused a severe disease in many young men, who became paralyzed and blind for many years. The human immunodeficiency virus (HIV) is the most perfidious one. Acting jointly with trichomonads and other pathogenic germs, it causes the AIDS-“the plaque of 20th century”.
The interaction between a trichomonad and its internal parasite resembles that between a human being and his internal parasite-the trichomonad. Indeed, when trichomonads begin to multiply with formation of a tumor, the human being also isolates them and creates a peculiar vacuole. Oncologists know it well: wherever a tumor appears, it is isolated from the human body by a capsule of immunocompetent cells.
To invade blood, some pathogenic germs may stick to the trichomonadal surface. To this end, they release an adhesive substance – fibronectin. This forms a microbial shell on the trichomonad surface. This shell protects the trichomonad from specific humoral and cell-mediated antibodies. As a result, the trichomonad can easily evade leukocyte attacks. When trichomonads come into blood from genitals, they carry mycoplasmas, ureaplasmas, cytomegaloviruses, and other pathogenic germs. The invasion of blood is mediated by the enzyme hyaluronidase. It dissolves the intercellular substance containing a hyaluronic acid.
In the middle of 20th century, parasitologists carried out interesting investigations with trichomonads, in which trichomonads were cultivated with spermatozoons. It was observed that spermatozoons slowed down near trichomonads. After that, the heads of spermatozoons began to dissolve, and one after another, the spermatozoons were pulled into the cytostome – a peculiar trichomonad’s mouth. When the trichomonad was engulfing one spermatozoon, it held some others with flagella. So, the trichomonad could engulf 5 spermatozoons at a time. It usually took 3 to 4 hours for the trichomonad to digest spermatozoons (or erythrocytes). After that, the parasite hunted for new preys.
The author of the Atlas also managed to observe predacious trichomonads under a microscope. The trichomonads were placed in a nutrient medium containing many bacteria. It was seen how a seemingly immobile flagellar trichomonad made a sudden lunge to capture a bacterium. Hence, trichomonads are quite dangerous for human beings. Besides the fact that they are dangerous by themselves, trichomonads can carry aggressive viruses and bacteria. It is the trichomonad that causes fatal illnesses, such as cancer, cardiovascular pathology, arthritis, multiple sclerosis, psoriasis, AIDS, and many others. Because of this, we need to be thoroughly familiar with this parasite. With this end in view, we shall first outline trichomonadal features and then discuss these features in more detail. We shall consider trichomonads at all stages of their existence: cystiform (sprout), amebiform (transient), and flagellar (vegitative).
The Atlas shows all vital cycles of trichomonads: at the initial stage, they are vaginal trichomonads, at the intermediate stage, they are blood parasites, and at the final stage, they are so-called tumor cells. Although trichomonads are polymorphic at all these stages (due to agamogenesis), they reveal a striking resemblance. This has to confound scientists trying to verify the common nature of parasitic trichomonads, undifferentiated blood cells, and so-called tumor cells. This will make it possible to establish the nature of cancer, infarction, and other fatal illnesses.
Let Me Introduce to You: Trichomonas!
Trichomonas is a genus of parasitic flagellate protozoa. It is attributed to the family Trichomonadidae of the class Polymastigina. This is an obligating zooblast. There are more than 100 species of Trichomonas. They are widespread in birds, wild and domestic animals, as well as in the cold-blooded creatures (such as amphibians and reptiles). The human body is inhabited by three species of Trichomonas: Trichomonas tenax, Trichomonas hominis, and Trichomonas vaginalis. They reside in the mouth, intestines, and vagina, respectively. Human trichomonads don’t form a cyst (a thick-walled protective membrane) even under living conditions adverse and dangerous to their life.
These parasites can perfectly adapt themselves to living in the human body protected by the immune system. Trichomonads can avoid immune reactions using a variety of methods. To this end, they can attach different germs and the host plasma to their surface; they can clean off antigens from their surface; and they can release proteins that are identical to the human ones. Under extreme conditions trichomonads are capable to be split into small protoplasmic particles. Such particles contain euchromatin and heterochromatin-substances of which the chromosomes are made. This enables trichomonads to preserve their species. Trichomonads never leave the host because they die in the air. When once trichomonads have invaded a human subject, they live in him unless he dies. Trichomonads extend their living-space and scope of influence by sexual transmittance. For the first time, a human subject can be infected with trichomonads in the womb of an infected mother. The embryo takes up parasites with amniotic fluid. A newborn can also be infected after childbirth. Trichomonads can be transmitted by a licked nipple, bitten banana, as well as by public tableware, bed-clothes, and bath.
For the first time, Trichomonas vaginalis was detected by French anatomist Donne in 1836. He detected this protozoan in the vaginal discharge of an infected woman. For a long time, this parasite was regarded as a harmless saprophyte that feeds on bacteria and dead organic matter. In 1870, I.Lazarevich was the first to describe the clinical picture of an inflamed uterine cervix. He pointed out that the local inflammation worsened an organism general state. Only in 1916, having analyzed clinical findings, Hoche pointed to the pathogenic effect of trichomonads.
In the prewar and postwar years, Soviet scientists established that Trichomonas vaginalis could exist not only on the vaginal wall, but in ulcers and also in the prostate gland. Moreover, Trichomonas vaginalis was detected in blood in 37 percent of cases. These facts motivated careful investigations of trichomonads, which were performed up to the early 1970s. The results of these studies enabled many researchers to become Doctors of Philosophy, Doctors of Sciences, Professors, and Academicians. With special respect, I should name V.Dogel’ and E.Pavlovsky, who wrote several textbooks on parasitology. The results of their studies were of great importance for medical science. In those postwar years, trichomoniasis became widespread and its treatment was a high-priority task. Unfortunately, these investigations were soon stopped unfinished. Owing to this, the researchers did not manage to disclose the main secret of flagellates – the progenitors of metazoans. This secret is that the Trichomonas is a “relative” of the human being. This parasite and the human being have a common parent-the primary flagellate. Presently, this parasite is the main biological enemy of mankind. It kills people by means of cancer, infarction, and AIDS.
Investigations of parasites were stopped owing to the genetic boom in medicine, which occurred in the 1960s. Because of this, many important results of population screening obtained by parasitologists were ignored. Thus, for example, between the late 1960s and the early 1970s, gynecologists and parasitologists conducted a widespread screening of women. It was found that the occurrence rate of sexual trichomoniasis in women recently confined was 34 percent, whereas that in expectant mothers was 35 percent. Of these, 51 percent were infected with trichomonads. These parasites were also detected in the genitals and rectum of one-day-old and two-day-old newborn infants. Urethritis was diagnosed in 67 percent of examined women, 40 percent of men, and 9 percent of girls.
Investigations were made on laboratory mice infected with a single injection of Trichomonas vaginalis into the peritoneum. In this investigations, the trichomonads were obtained from infected human subjects. Depending on the injection dose and parasite pathogenicity, trichomonads caused the animal death, internal-organ and lymphatic-node destruction, or connective tissue proliferation. Unfortunately, the last observation has not been identified with such human reactions to neoplasm growth. However, such neoplasms are well known because tumors and blood clots are always encapsulated in connective tissue.
For the first time, Trichomonas hominis was detected by Wenyon in 1926. This parasite has a cytostome, which enables it to sequentially engulf up to three erythrocytes. Trichomonas hominis can devour erythrocytes either in the host or in cultural media. When Trichomonas hominis invades the blood, it may cause anemia. Some 50 years ago, these parasites were established to cause hemocolitis, colitis, entercolitis, and cholecystitis. These diseases are accompanied by development of edemas, erosions, polyps, and ulcers in the intestinal path. Unfortunately, ulcers were not also identified with precancer. Trichomonadal and oncological patients exhibit common symptoms, such as pale skin, pale mucous membranes, loss of weight, anemia, loss of strength, reduced immunologic tolerance, and reduced ability to work.
Trichomonas tenax is the least studied species. It is often detected in the mouth and respiratory tract. It can be found in the phlegm, tonsils, gingival pockets, conjunctiva of the eyeball, gangrene-stricken regions of the lung, and blood. An examination of patients with purulent diseases and malignant lung neoplasms revealed the presence of flagellar trichomonads in some patients. In the 1970s, a population screening of the mouth showed that trichomonads were detected in the ginigval pockets of 49 percent of the patients.
Trichomoniasis was studied in domestic animals. It was found that this infection caused severe diseases such as palsy, gastroenteritis, arthritis, infertility, spontaneous abortion, as well as changes in hepatic tissues and other organs.
However, all these observations and statistical data were understated. They did not represent the real picture. In native preparations, trichomonads were detected under a microscope by their mobility. In fixed preparations, they were detected by the presence of flagella or nuclei. However, trichomonads can easily change to an unrecognizable cystiform or amebiform without flagella. This can be caused by drugs, immune reactions, pathogenic germs, nutriment alterations, or other adverse conditions. In this case, it is difficult to differentiate trichomonads from lymphoid and other cells. As a result, they are not detected, even if they are present in large numbers.
Of the three species of trichomonads, Trichomonas tenax is the most widespread one. It causes periodontal diseases and caries of teeth, which are the most well-known clinical manifestations of this parasite. However, this species exhibits the least aggression, which was demonstrated in experiments on mice. To this end, different species of trichomonads (obtained from the human being) were inoculated into the abdominal cavity of mice. It was found that the destruction of internal organs by 4 million Trichomonas vaginalis was similar to that by 25 million Trichomonas hominis and 100 million Trichomonas tenax.
Probably, this motivated parasitologists to perform active investigations of Trichomonas vaginalis. This protozoan is the largest, most active, and most pathogenic one. In the 1960s, this species was involved in many experiments, whose results enabled many researchers to receive their Doctor’s Degrees. However, the scientists soon disaccorded. Some of them considered trichomonads to be harmless and useful. They thought that this parasite fed on pathogenic bacteria and dead organic matter. But, they left out of account that trichomonads could melt cells with toxic enzymes. The other scientists considered trichomonads to be harmful. They thought that this parasite was dangerous for human health. Most scientists believed that trichomonads caused local genitourinary diseases. Most of those specialists thought that trichomoniasis was mainly a sexually transmitted disease (STD). As a result, in 1958, at the First All-Union Congress of Dermatovenereologists, Estonian physicians suggested that trichomoniasis should be classified as an STD.
However, their proposal was rejected because it might have caused family quarrels. In this case, physicians had to treat not only a woman, affected by trichomonadal colpitis, but also her husband, who considered himself to be absolutely healthy. Strange as it is, the disease was often transmitted by men, who became unfaithful to their wives. However, sluggish cystiform trichomonads, residing in the male genitals, did not cause acute diseases in them. As a result, the men were calm. They were surprised when their wives began to worry.
However, the indifference of men to trichomonads produced a latent effect. The point is that the immune system did not react to cystiform (or so-called sprout) trichomonads. As a result, these parasites spread from the urethra to the upper regions of genitals and invaded blood. Trichomonads multiplied in the blood and formed thrombus colonies. This brought about constriction and occlusion of blood vessels. Later, this led to early impotence or infarction, to which men were more predisposed than women. Hence, trichomonad manifestations in women (such as colpitis discharges and others) were evidence of insensible, but progressive, diseases in their husbands.
Men, especially those in office, should know about it because they establish medical and national policies. And national welfare and health should be the most high-priority tasks.
In the 1960s, medical specialists and experts were convinced that trichomonads were harmless. As a result, when young sciences (such as genetics, virology, and immunology) were developed, many research projects on parasitic protozoa were closed. Investigations on trichomonads suffered the same fate. Many specialists had to be trained for a new profession. Since physicians left Trichomonas without control, this parasite survived. In 1975, trichomoniasis was classified according to the International Statistical Classification of Diseases as Infectious and Parasitic Diseases. Later, Trichomonas was found to cause the first stage of precancer, followed by cancer and other dreadful diseases.
To stop investigations of parasites was a serious error made by medicine in the 1970s. Scientists should have been more watchful because trichomonads were detected in the absolutely sterile blood. Moreover, trichomonads were the only protozoa capable of surviving in human genitals. Investigations demonstrated that these parasites caused infertility and spontaneous abortion in animals. Hence, they could produce similar effects in human beings. All these facts (as well as deteriorated human health, reduced life expectancy, and agonizing death of fatal illnesses) motivated us to revive in-depth investigations of the pathogenic effect of trichomonads on human health, life expectancy, and reproduction.
A need for such investigations has also been confirmed by the results of population screening for Trichomonas tenax and Trichomonas vaginalis. The screening was carried out several years ago with the assistance of Tamara Svishcheva. It was performed on stomatological patients with gingival pockets, whose age was between 21 and 82. The results obtained showed that all of the examined patients had trichomonadal colonies. They were represented by small whitish nubbins. Being cultivated in a nutrient medium, these colonies divided into separate elements. Some of them grew and became amebiform or fusiform (followed by the flagellar form).
Another study was made in women at the age of 16 to 58, who had sexual problems. It was found that Trichomonas vaginalis was present in all these women. Most often, this parasite was cystiform and vacuolized. It was partially destroyed by numerous bacteria and fungi. Presently, genuine trichomoniasis is encountered in few women. This disease is characterized by a minimum of microflora and a maximum of trichomoniads, the flagellar ones included. Because of this, the number of patients suffering from trichomonadal colpitis (characterized by acrid vaginal discharges) is decreasing. This results from the presence of pathogenic germs in the vagina. As a result, trichomonads have to rescue themselves: they penetrate tissues, blood vessels, and the upper organs of the body. As soon as trichomonads get into a more favorable environment, they begin to multiply. This gives rise to cancer, thrombosis, and other severe diseases.
Blood Variation in Course of Time
Evolution of Human Diseases in the 20th Century
In the beginning of the 20th century, cancer accounted for only 3 percent of other illnesses. At that time, mankind was threatened by epidemics of plaque, cholera, smallpox, typhoid, and anthrax. Although scientists overcame these mortal epidemics, they made way for new insidious diseases. Acting gradually and imperceptibly, these maladies spread around the world over the last century. In the 1990s, Russia saw a large increase in cancer patients. The cancer incidence reached 30 percent. As a result, cancer ranked second among other mass diseases. Sad superiority belongs to cardiovascular diseases. On the third place there is a diabetes, further there is a stroke, bronchial asthma, arthritis, multiple sclerosis, psoriasis, and other incurable diseases. Strange as it is, the actual causes of these diseases remain unknown. Because of this, these maladies are incurable, their early diagnostics and effective prophylaxis are impracticable.
Doctor Olga Eliseeva has advanced her own theory of cancer development. It is based on the action of fungi and parasites. Parasites are organized creatures. They develop gradually. The tapeworm Echinococcus can cause large tumors that grow through the liver, lungs, peritoneum, and brain. Other helminths were also detected in tumor structures. It is surprising that classical medicine does not understand it.
Chemotherapy in a root is wrong, it is harmful. Why do living cells begin to multiply and form a tumor? Is an organism its own enemy? However, all chemotherapeutic procedures are based on the destruction of own cells of the human being. For example, lung tumors are treated with drug compounds that destroy human cells. As a result, chemotherapy leads to intoxication, immune suppression, and human death.
The structure of a cancer tumor is made by microorganisms. The tumor composition depends on the cells that have been eaten by a fungus. Some fungi feed on tissues of the breast gland, lung, and liver, whereas the others feed on tissues of lymphatic nodes. Because of this, tumors differ in their composition and shape. Why do not oncologists see it? This is because they examine histology, not morphology. Oncologists make microscopic cuts of a tumor while there it is impossible to obtain and completely to see a mycelium cells.
Once, when anybody was making a report at a symposium, a surgeon (otolaryngologist) stood up and said: “During all life, I operate the maxillary sinuses. But, in my life I have never seen a parasite there”. Suddenly, a woman microbiologist, Doctor of Medical Sciences, has promptly appeared on a tribune. She said: “In our experiments, surgeons gave us a substrate taken from the sinuses. We put it on a nutrient medium and waited for a while. As a result, we saw both fungi, and parasitic larvae, and helminthoid eggs. It was a complex infection”. The surgeon was depressed and went back to his seat. A year later, they met each other. And the surgeon said: “You were right. Morphologically, there are plenty of creatures: from helminths to protozoa and metazoans. They crawl and clamber”.
Secret of Birthmarks
Birthmarks are growths on the skin formed before birth. However, why do people so dislike and fear them? They know that a damaged birthmark may have grave consequences. Doctor Olga Eliseeva examined birthmarks in people by means of the Vegetative Resonance Diagnostics (VRD) technique. She found that parasitic larvae (such as trichina and schistosoma) resided inside birthmarks, whereas fungus (such as Aspergillus niger and Aspergillus fumigatus) lived near the skin surface. From above, birthmarks were covered with pigment cells - melanocytes. It was concluded that the placenta could not always protect the fetus during pregnancy. As a result, the fetus tried to move isolated parasites, which had passed through the placenta, away from vital organs. Due to this, the parasites found themselves near the skin. Helminth larvae, which are spread mainly via lymphatic channels, were moved away to the subcutaneous region. The most hazardous fungi Aspergillus, which inhabit blood vessels, were moved away to the cutaneous region. Because of this, the larvae and fungi resided in peripheral vascular plexuses. The parasites “sleep” peacefully in their dwelling places unless they are disturbed. However, they can be disturbed, for example, by solar radiation. To protect himself from solar radiation, the fetus covers the parasites with pigment cells. When the protection fails and sun rays disturb the fungi Aspergillus, they begin to develop, multiply, and spread. The fungi prefer to inhabit blood vessels and enthrall pigment cells. As a result, they can spread over the entire body with enthralled melanin. When birthmark walls are damaged (by an injury, puncture, operation, or irradiation), the parasites begin to multiply. After that, they move to their favorite places, carrying or not carrying pigment cells. In a situation like this, the histological examination of an affected node will be more difficult to understand. When parasites contain pigment cells, histologists will set a diagnosis of melanoma (cancer). In this case, unless the patient is treated for parasites, he or she dies slowly. In a severe case, when the patient’s immunity is exhausted, helminths or fungi spread over the entire body. When they affect the brain, the patient dies a sudden death - the “pharaoh vengeance”.
Secret Agent of Cancer: Trichina
Trichinae are small round worms. They are viviparous worms of two sexes. A female worm is about 4 mm in length, whereas a male worm is about 1.6 mm in length. These worms may cause a disease in man - trichinosis. Trichinae are met in different omnivorous and raptorial mammals. They are transmitted by domestic and wild animals. The human being is invaded by eating raw or underdone meat of domestic or wild animals, such as the swine, badger, bear, seal, and walrus. The sale of pork not examined by veterinarians favors the trichinosis spread. The infection can be transmitted via lard, ham, and sausage. Once, I had a heart-to-heart talk with a saleswoman. I asked her: “In which way do you check your meat for worms?” And she replied: “In no way! We pick out the worms we see. And then we sell the meat”. Everything was simple and easy. Pubescent trichinae live in the small intestine for 6 to 8 weeks, whereas larval trichinae can reside in muscular and lymphatic tissues for tens (!) of years. So, larval trichinae can live in the host - man or animal - during all its life. They can invade an organism at the larval stage only.
The last several years have seen a large increase in the trichina infection incidence. The VRD technique revealed trichina worms in every other man. Trichinosis is particularly widespread in big cities. This is related to keenness on the pork shashlik (kebab). A changed recipe of shashlik preparation additionally favors the trichinosis spread. So, some cooks soak pork in kefir, not in vinegar. They say that shashlik prepared in this way tastes more delicious. Surely, it tastes more delicious. However, in this case, the meat has not been disinfected by the acetic acid. As a result, the trichina larvae remain alive.
What stimulates trichina reproduction? The larval cyst can be destroyed or damaged by mechanical actions. For example, these actions can be as follows:
- Trauma (such as bruises, scratches, or wounds). Clinical practitioners know that a trauma can stimulate the development of tumor metastases.
- Puncture (a small hole made by a sharp object for histological examination). A puncture can also destroy the larval cyst.
- Surgery. An ideally performed operation, which failed to have eliminated other parasitic conglomerations in the body, may cause trichinae to multiply. A majority of surgeons would operate both benign and malignant tumors. Oncologists do the same: they see a tumor, make a puncture, and perform a histological examination. On seeing atypical cells, they set a diagnosis of cancer. Hence, the patient should be operated on. However, the cyst may encapsulate not only the larva but also many other germs and cell structures. As a result, the histological examination will yield an absolutely unclear result, which will be interpreted as cancer. The patient will be directed to operation, radiotherapy, or chemotherapy. However, the operation will spread the larvae and enhance aggression of mature parasites inhabiting intestines.
- Electrophysiotherapy. It may either crack or destroy the cyst, which will cause larvae to spread. Oncologists observed that physiotherapeutic procedures stimulated the development and spread of tumors. Because of this, they intuitively prohibited their patients from undergoing physiotherapeutic treatment.
- Acupuncture. An inexperienced acupuncturist may break the parasitic conglomeration. In the European countries, oncologists intuitively banned this treatment for cancer patients. In China, acupuncture is approved for such patients. However, a Chinese apprentice is allowed to practice after two-year learning.
- Sauna. Heat causes blood vessels to dilate. When the cyst is surrounded by inflammatory regions, heat may enhance the inflow of leukocytes. This will exacerbate inflammatory reactions. As a result, the vascular wall can dissolve, and the cyst can break.
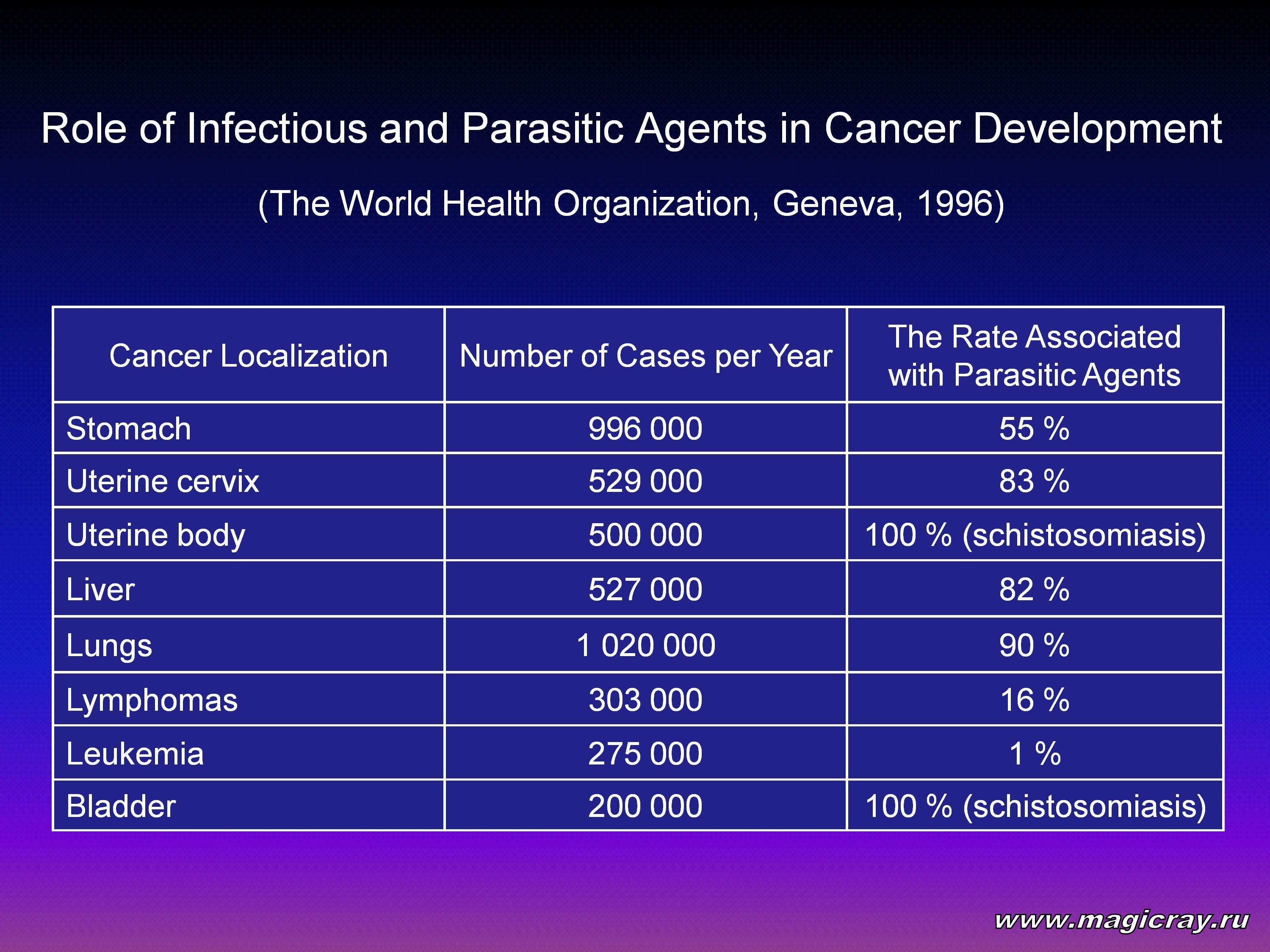
In this connection, no matter how sophisticated carcinogenic mechanisms are, we cannot reject the existing theories. This has been proven by the World Health Organization statistics, based on the verified causes of cancer (Geneva, 1996).
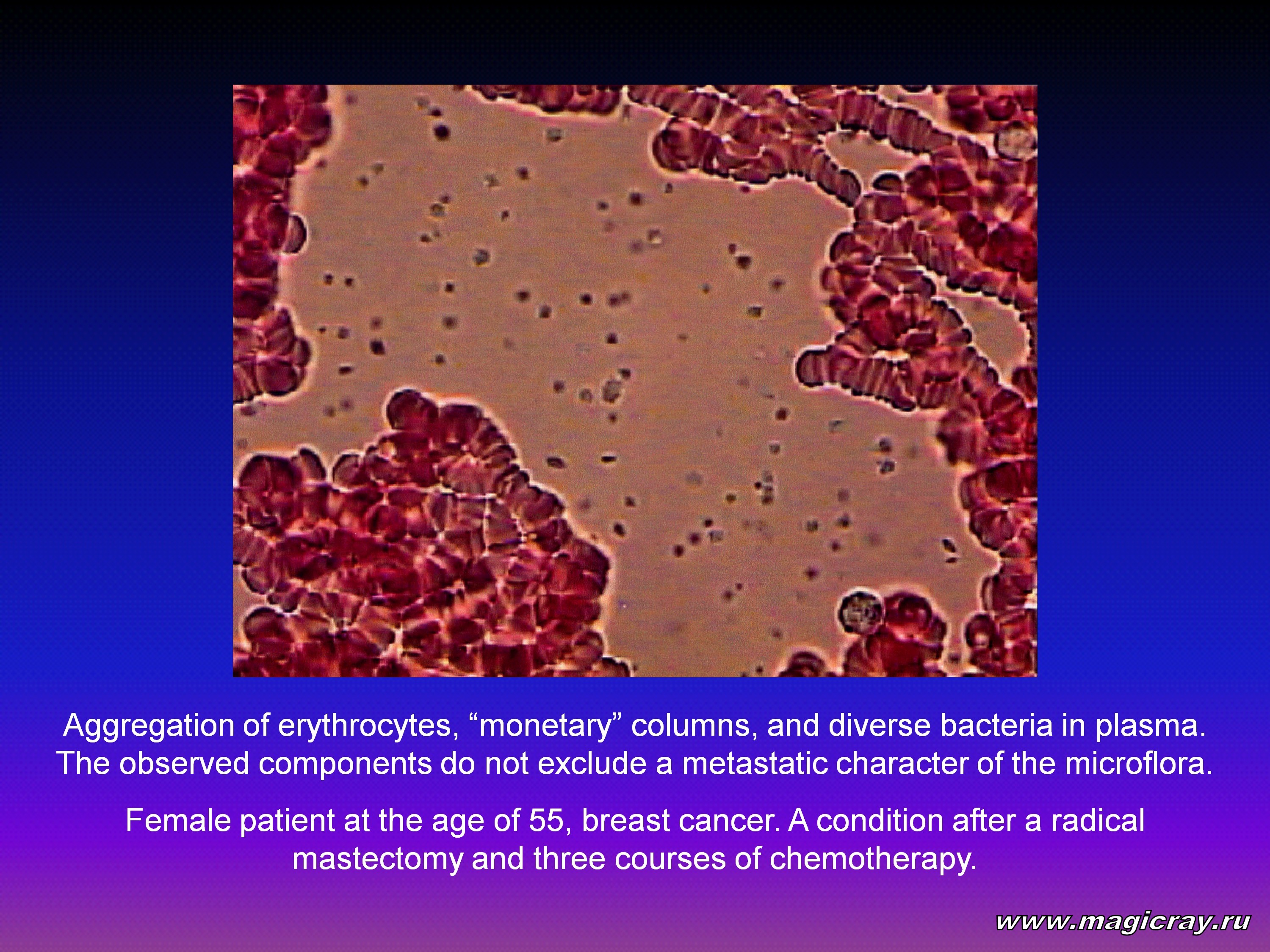
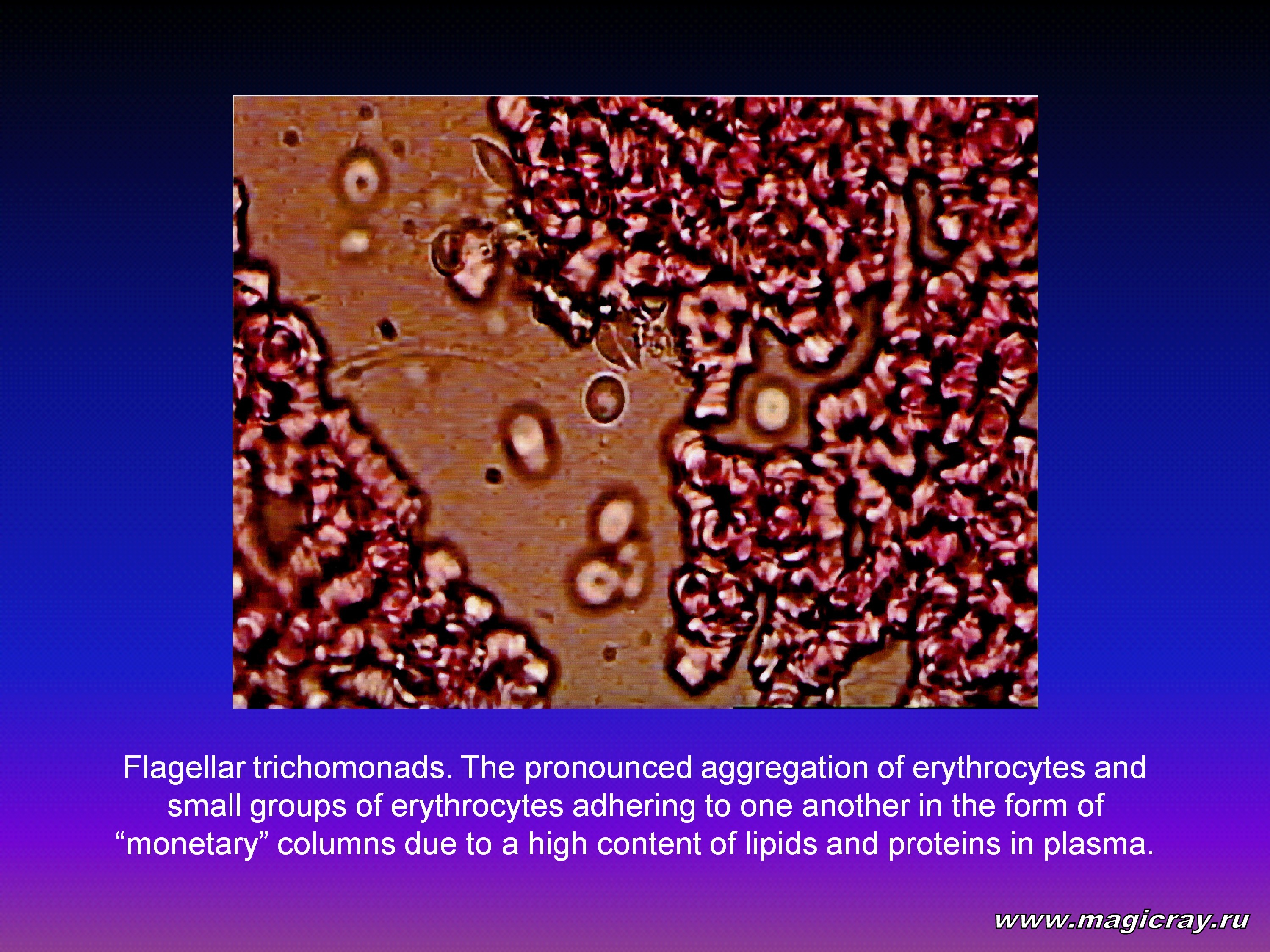
At present, Doctor Marina Soshenko is carrying out investigations on the living blood drops by the scanning microscopy technique at our clinic. When Tamara Svishcheva and I consulted our living blood samples, we concluded that different diseases (such as cancer, diabetes mellitus, eye melanoma, and vascular disorders) differed in the intoxication degrees and microbial, helminthoid, and trichomonadal invasions of blood cells.
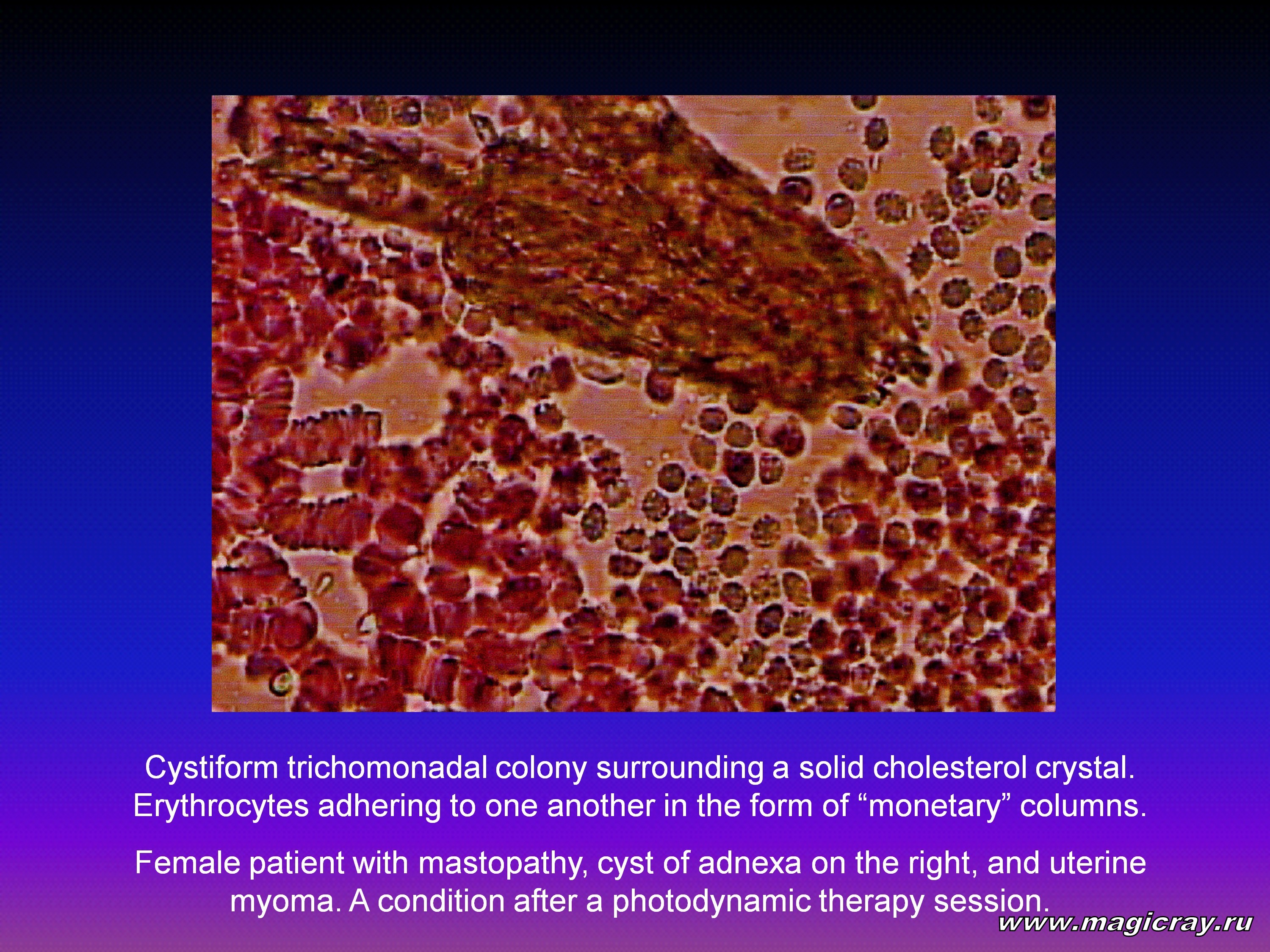
Besides that, a PDT session and laser therapy session were found to clear blood and lymph from solid cholesterol. They were also found to activate the immune system. These therapies set lymphocytes in active motion. Moreover, after the treatments, lymphocytes opened their cellular membranes to capture alien agents. In our previous investigations, we studied low-level laser therapy mechanisms. These investigations were made on laboratory rats. To this end, laser radiation influenced the lymphatic vessels of the mesentery and lymphatic collectors of the myocardium. The obtained results revealed that laser radiation activated the lymphatic system of the animals. Further experiments were performed in patients with different chronic diseases. To this end, laser radiation influenced the projection zones of different organs on the iris. The obtained results showed that laser radiation produced a lymph-stimulating effect. We patented a technique for a patient’s noninvasive detoxication - iridoreflexotherapy.
The obtained results allowed us to develop a technique for activating physiological drainage systems, such as the gall bladder, liver, kidneys, skin, and lungs. The technique relies on the control of a living blood drop. To this end, the blood drop is scanned before a PDT session. The proposed technique runs as follows:
Preparatory Stage
- Sango Coral – 1 packet: dissolve it in 1 liter of water (in winter), or in 1.5 liter of water (in summer).
- Microhydrin – at the age of 20 to 40 years: half a capsule twice a day (in the morning and in the evening), or 1 capsule once a day (in the morning); at the age of over 40: one-fourth, one-third of a capsule twice a day.
- Crystal Energy – 5 to 8 drops: add them to 1 glass of water or other beverages (except for coffee and alcohol).
Bile Duct Drainage
Repeatedly once a month
To recover the bile duct passage, the patient should take the No-spa drug compound before going to bed. He or she should take 1 or 2 pills with hot tea containing honey. This recovers the passage via Oddi’s and Lutkens’ sphincter. In the morning, the patient should take:
- Magnesia sulfate of 33 % (30-ml solution or 2 ampoules).
- Sorbite (2 tablespoons melted in 100 ml of hot water).
- Vegetable oil of 50 ml with a juice of half a lemon.
- Egg yolk – 1-2 pcs.
- Acidic mineral water such as Essentuki №4 or 17 – 100-200 ml.
These ingredients should be taken sequentially on an empty stomach at an interval of 30 min. After taking each component, the patient should lie on his or her right-hand side on a hot-water bottle. The bile duct is drained on an empty stomach once a month. The patient may have a loose stool during the treatment. It is recommended that the patient should be on a vegetable and sour-milk diet.
Liver Depuration (in 2 days)
Repeatedly once a quarter (=3 months)
On the liver-depuration day, the patient should not take meat, coffee, chocolate, cakes, and garlic. The liver-depuration procedure consists of 3 sessions. They are performed at an interval of 3 or 7 days. On the liver-depuration day, the patient should have his or her final meal at 06:00 p.m. After that, the treatment runs as follows:
- At 10:00 p.m., the patient takes 8 to 10 drops of a Valeriana’s tincture, mixed with a one-fourth full glass of water.
- At 10:15 p.m., he or she takes 2 Allohol pills.
- At 10:30 p.m., the patient mixes 30-50 ml of brandy with 30-50 ml of castor oil, followed by one-grapefruit juice. After that, the patient applies a hot-water bottle to his or her right-hand side for an hour or for an hour and a half. Before going to bed, the patient takes a Magnesium sulfate (1 teaspoon per glass of water).
- On the next morning, the patient takes the Enterosgel compound (1 tablespoon per glass of water).
Anti-helminthic Treatment
- Before going to bed, the patient takes the Helmintox compound (according to the prescription). In the morning, he or she takes a laxative (1 tablespoon of Magnesium sulfate).
- Before going to bed, the patient takes 1 Decaris pill. In the morning, he or she takes a laxative.
- Before going to bed, the patient should take 2 Vermox (Mebendazole) pills for 3 days. In the morning, he or she takes a laxative.
- The patient takes Biltricide (Praziquantel) according to the prescription, followed by a laxative in the morning.
- The patient takes Albendasol according to the prescription, followed by a laxative in the morning.
- The patient takes 5-8 Helmintosan pills daily for 1 month.
Anti-viral and Anti-mycotic Therapy
- Colloidal Silver – 1 teaspoon in the morning for 14 days, followed by a 10-day break, then 1 teaspoon in the morning for 14 days.
- C-Free – according to the prescription (2 packages) for 1 month.
- Pau D’Arco Bark – 3 capsules twice a day permanently.
- Black Walnut Leaves – 1 capsule twice a day for 1 month.
|
