10. Photodynamic Therapy for Skin Cancer of Inconvenient Localizations
A.A.Radaev, E.Ph.Stranadko, M.V.Riabov, T.M.Ibragimov
Introduction
Skin cancer is a most wide-spread type of cancer all over the world, and its frequency is constantly increasing along with the growth of the average life-time of the planet population. Every year the frequency of basal-cell carcinoma increases up to 3 to 6% in all industrially developed countries. The frequency of squamous-cell carcinoma also increases every year up to 3 to 10 % [1, 2]. As to the frequency of skin cancer in Russia, it has been second among malignant neoplasms since 2001. The increase of skin cancer frequency within 10 years (1996-2005) made 27.23 % [3], while in 2005 the absolute number of those with all types of malignant neoplasms was only 13.7 % higher than in 1995. The 60,763 new cases of skin cancer were diagnosed in 2005.
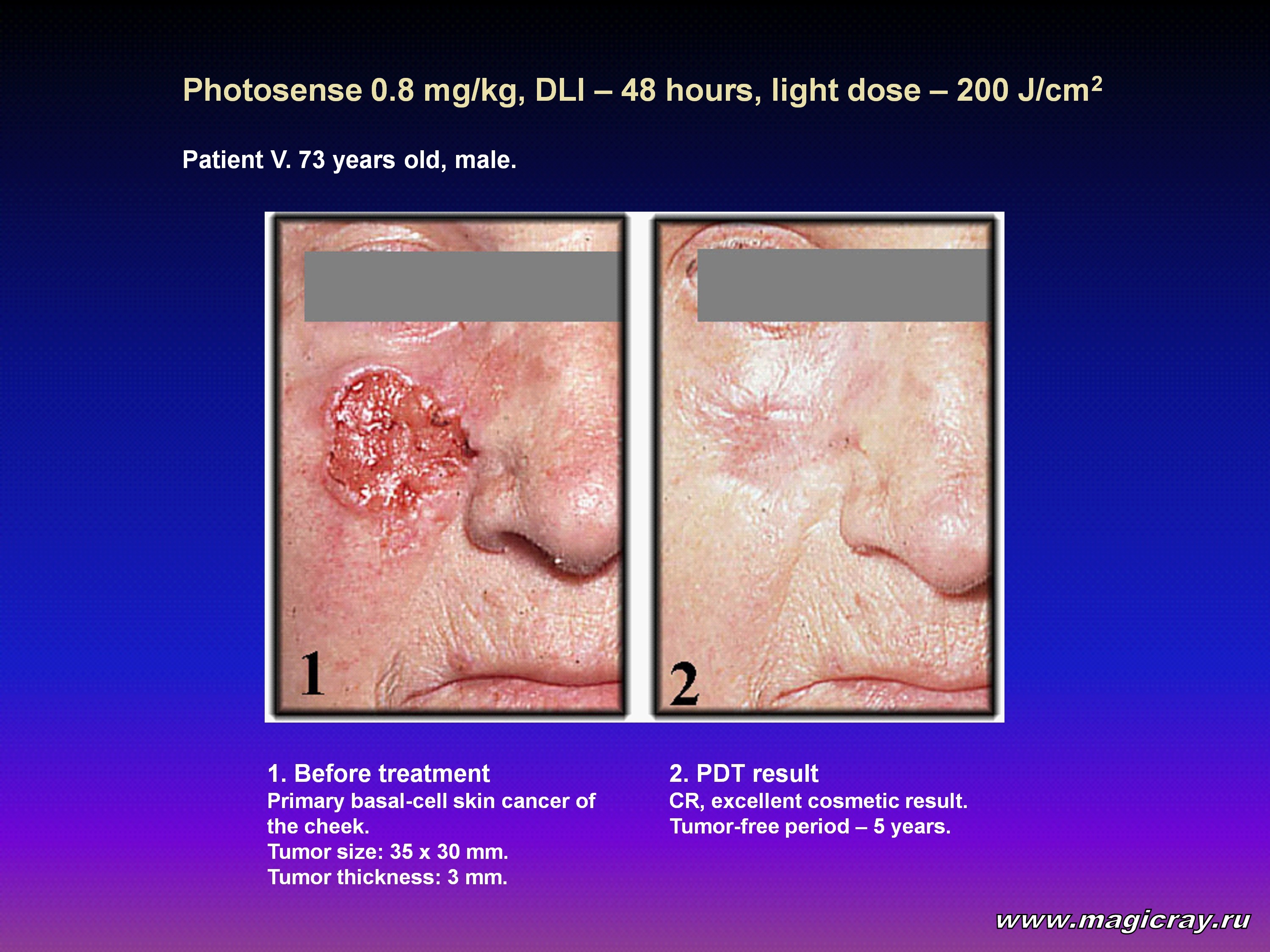
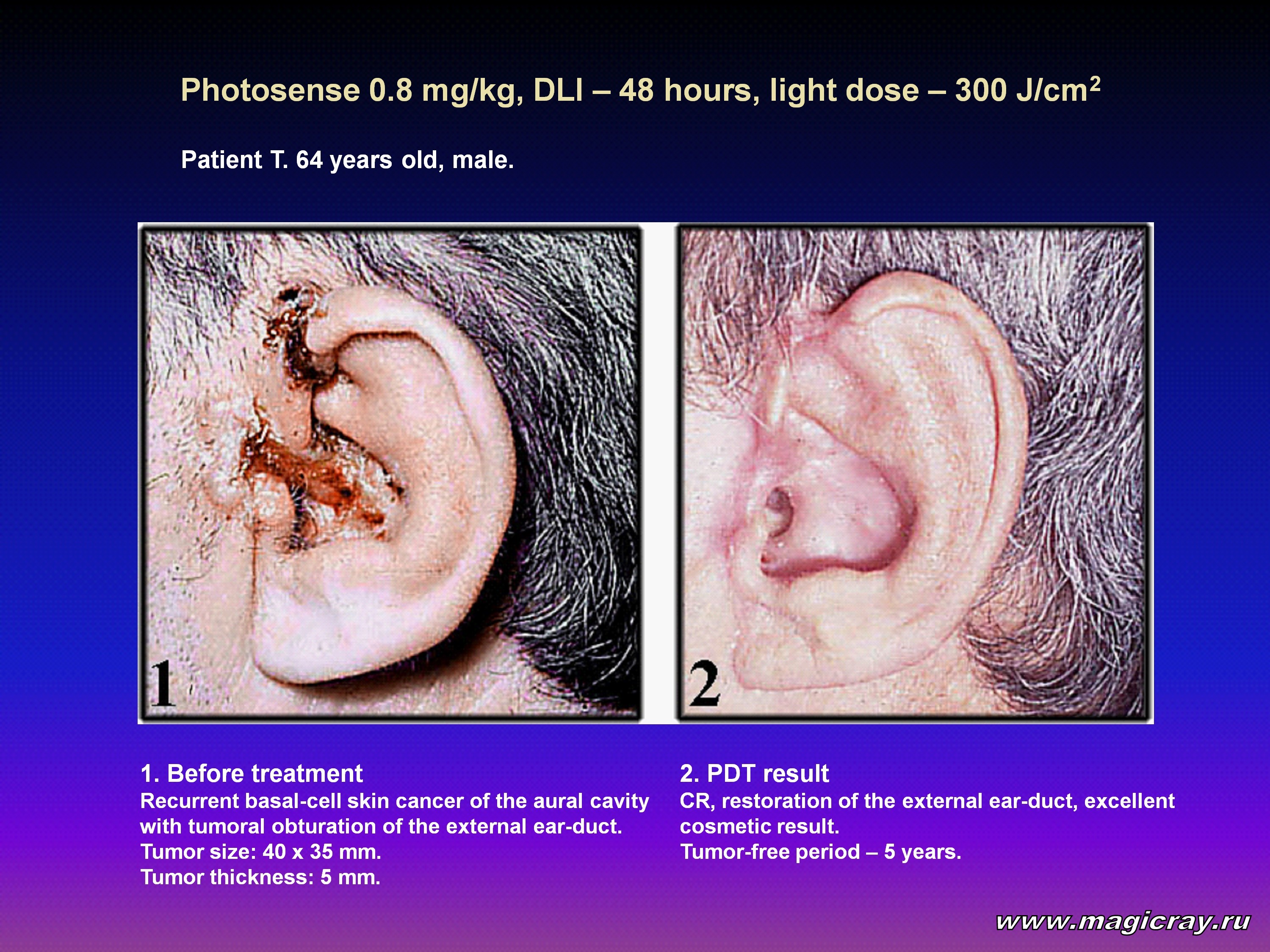
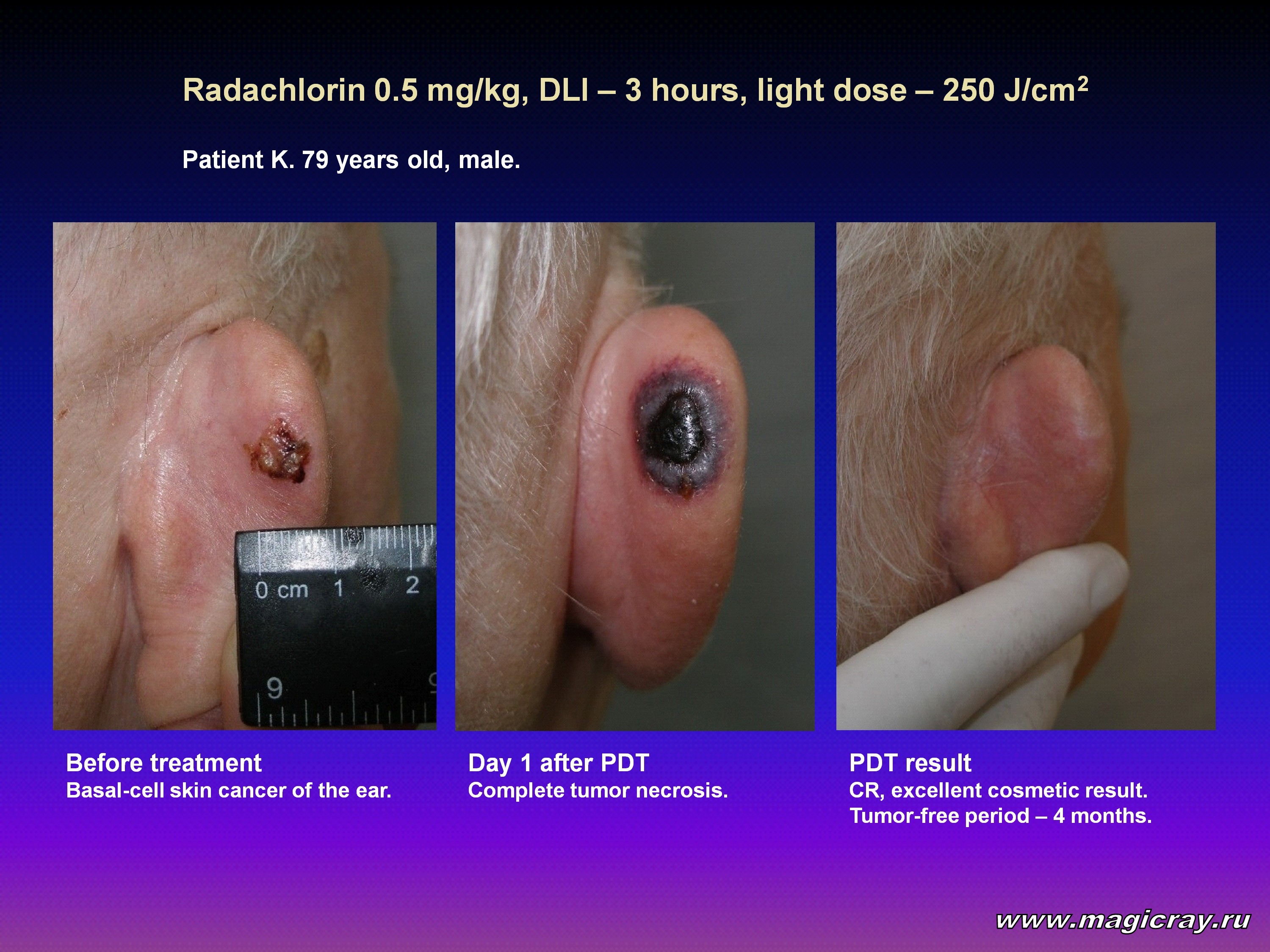
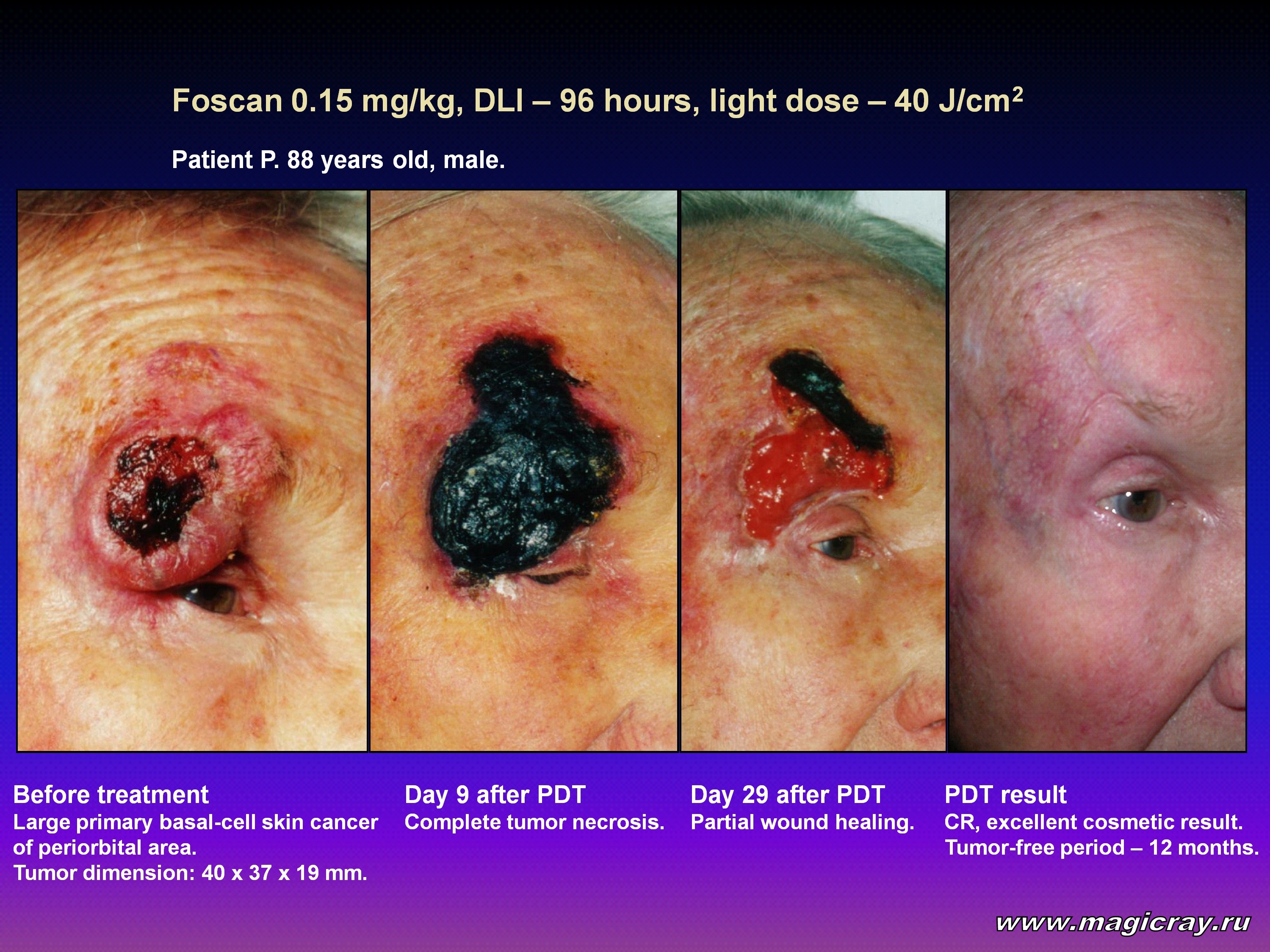
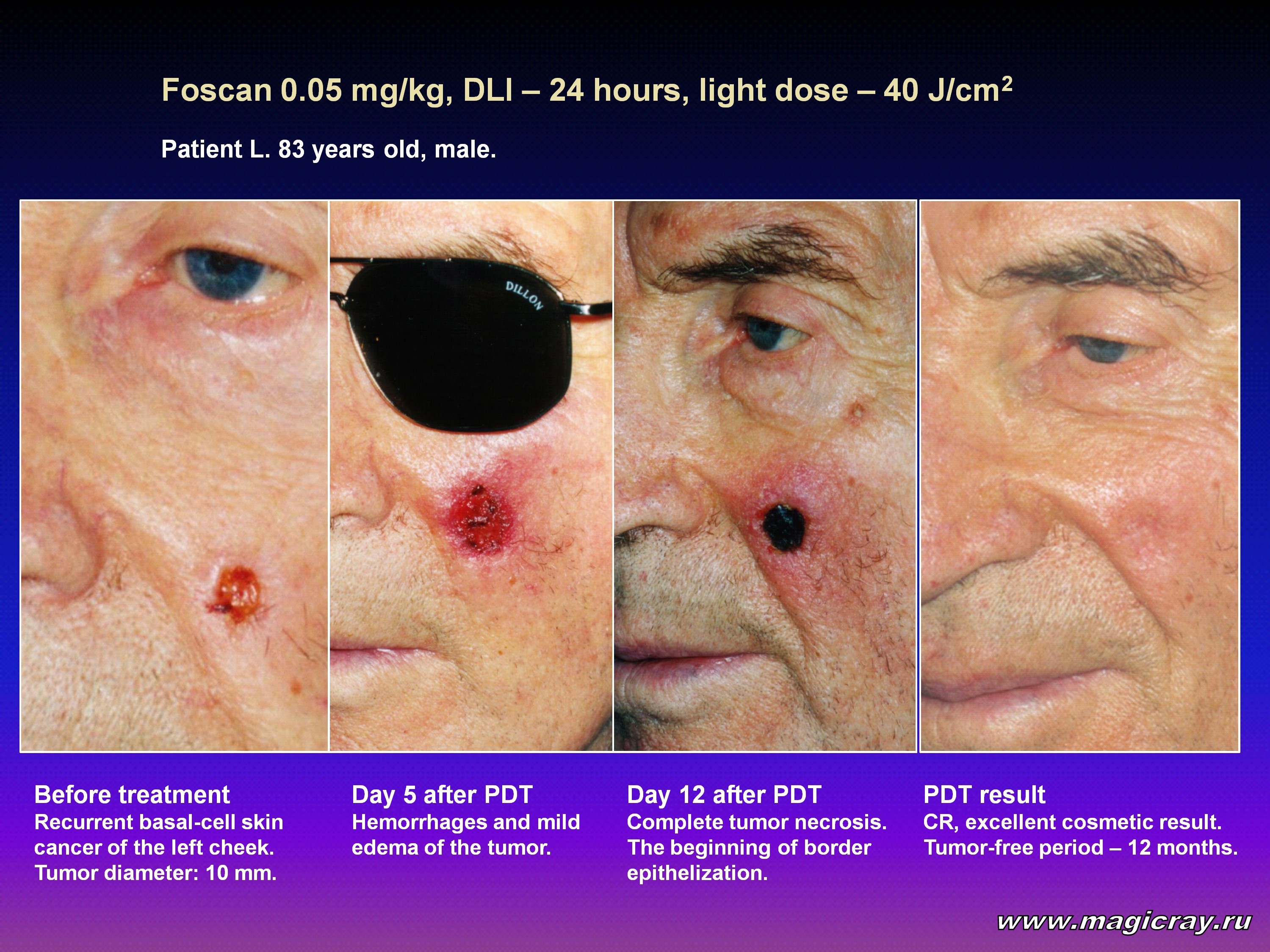
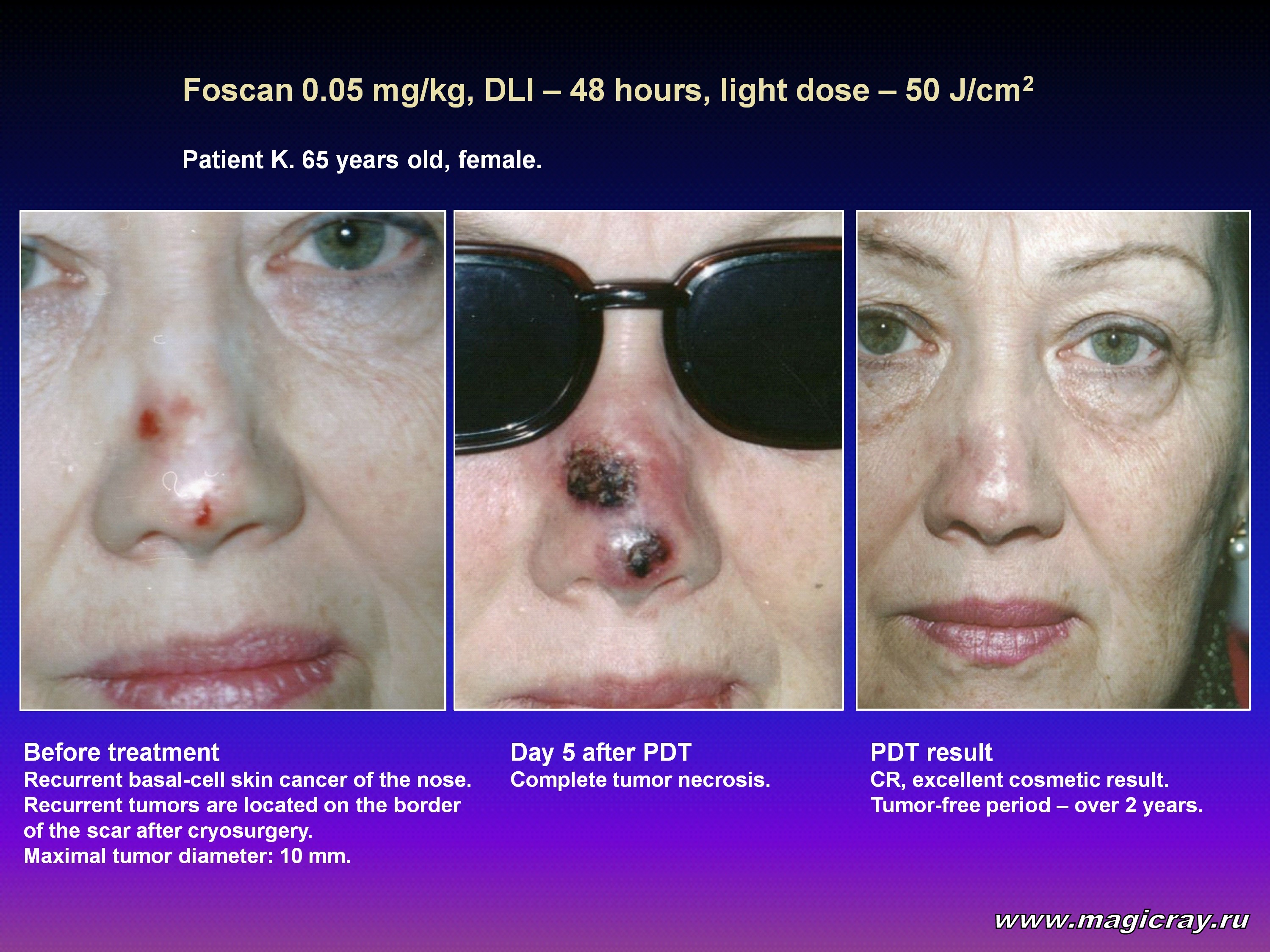
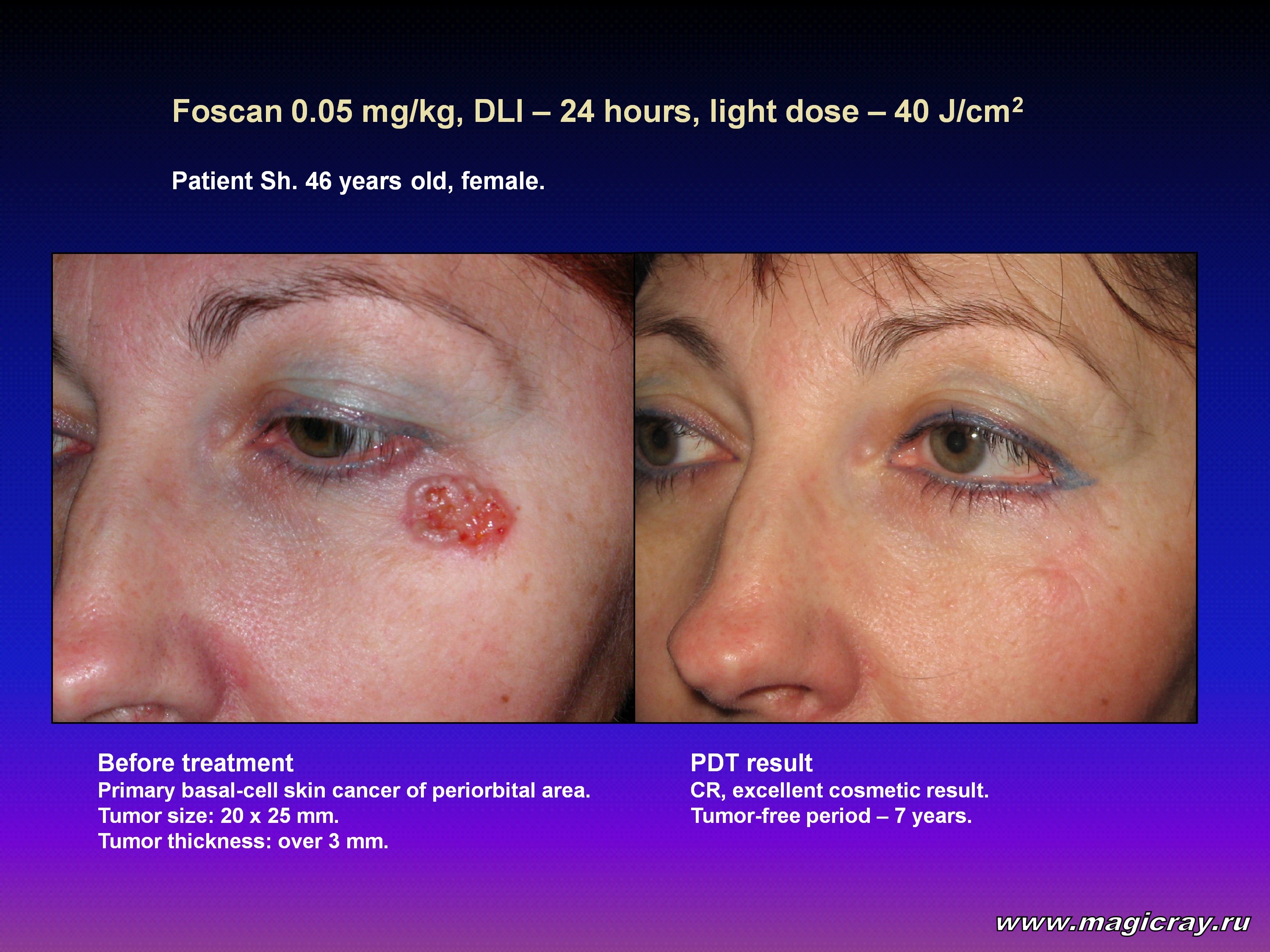
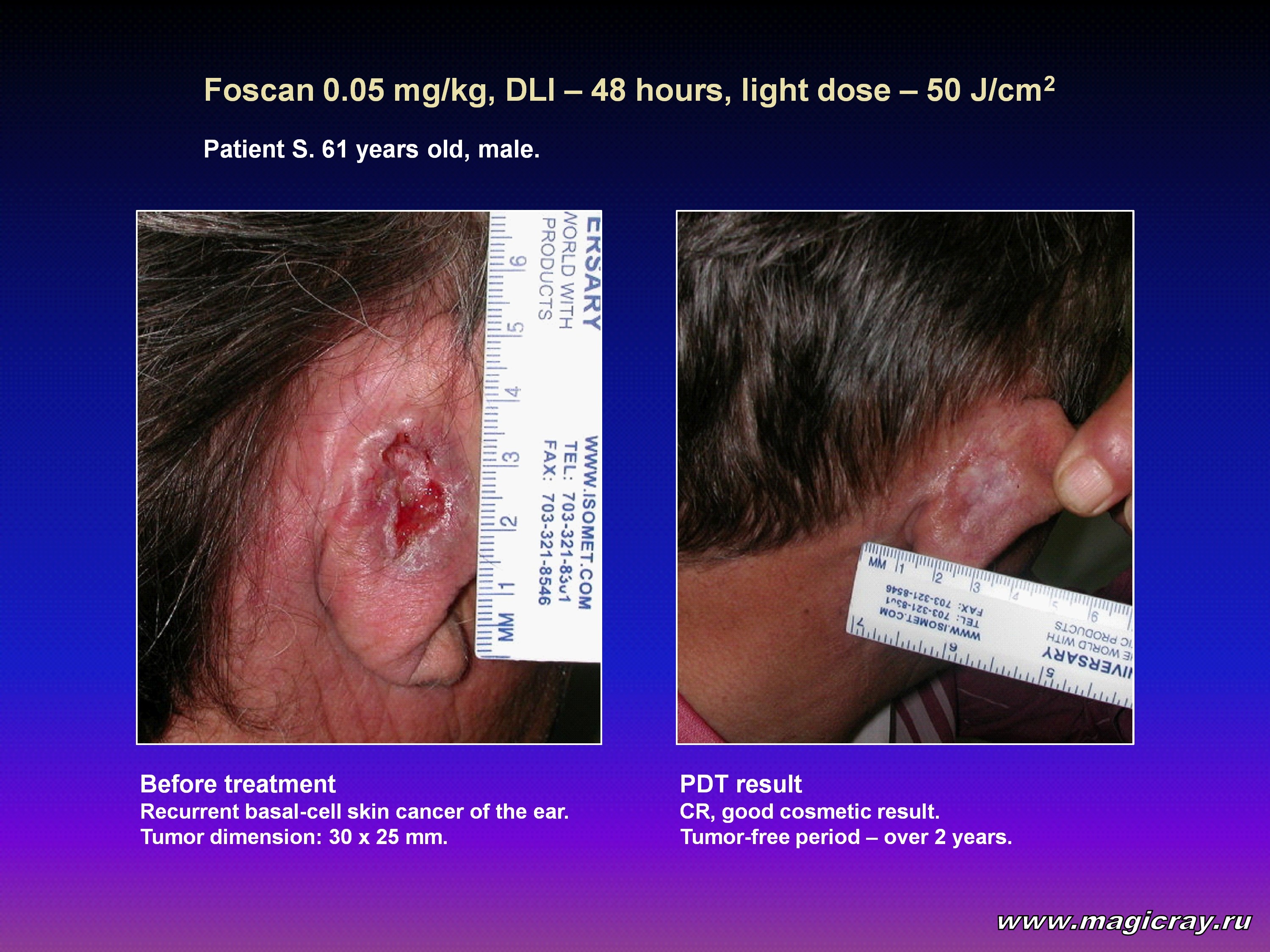
The traditional methods of skin cancer treatment are surgical excision and close-focus X-ray treatment. However, in case of inconvenient localizations, e.g. skin cancer on a face, aural cavities, the hairy part of a head, and also in case of multiple tumors, these methods are not applicable or bring about complicated functional and cosmetic defects. In this regard, inconvenient localizations are eyelids, the tails of eyes, the wings of a nose, nasal-and-labial folds, aural cavities, and an external ear-duct. The problem consists of that from 70 up to 80 % of skin cancer is localized on the head and neck, and 30 to 40 % of foci may be regarded as inconvenient localizations.
A minimally invasive and organ saving method of treatment – photodynamic therapy (PDT) – opens up new opportunities for the treatment of inconvenient localizations of skin cancer.
Materials and methods
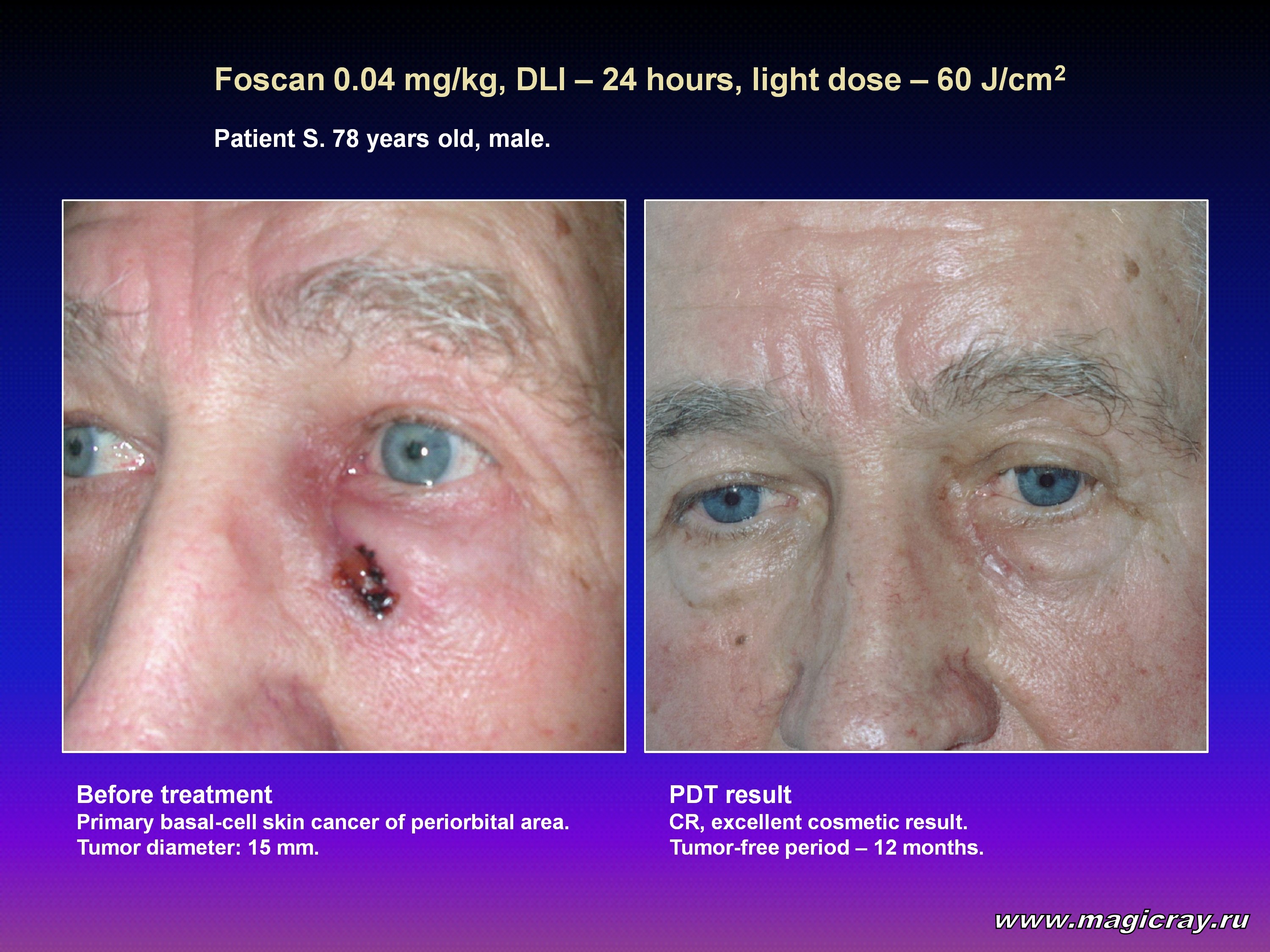
We studied 104 patients with skin cancer of inconvenient localizations (on eyelids or periorbital areas, on a nose, in the area of nasal-and-labial folds, on aural cavities and on the skin of an external ear-duct). The age of the patients was from 34 to 88 with an overwhelming number of elderly people, especially in the group of patients with recurrent cancer. 66 people were men, and 38 were women. Primary cancer was diagnosed in 47 patients. 57 patients had recurrent cancer after the treatment applied to them earlier (surgery, close-focus X-ray treatment, cryodestruction, electro- and laser coagulation). 93 patients were diagnosed with basal-cell carcinoma, 6 – with squamous-cell carcinoma, 4 – with metatypical carcinoma and 1 – with low differentiated carcinoma. The tumors of 46 patients invaded the cartilage and bone structures of a nose and an aural cavity; in 8 of these cases tumors penetrated into the nasal cavity (6 patients had the destruction of the structures of the external nose and nasal septum). In 14 cases there was an associated affect of an aural cavity and an external ear-duct, and the neoplasm process of 1 patient with recurrent cancer had reached the middle ear.
For PDT sessions we used domestic photosensitizers (Photohem, Photosense, Photoditazine and Radachlorin), as well as Photolon made by the Belorussian “Belmedpreparaty” company, and Foscan (temoporfin) made by the German “Biolitec AG” firm (Jena, Germany). For irradiation of tumors we used laser machines with a wavelength that corresponded to the absorption peak of a photosensitizer: for Photohem it was 630 nm, for Photosense – 675 nm, for chlorin photosensitizers (Photoditazine, Radachlorin, Photolon, Foscan) it was 662 nm.
Results
The therapeutic effect was achieved in all patients who had been treated (Table 1).
Table 1. Efficacy of PDT for primary and recurrent cancer of inconvenient localizations
Kind of pathology
|
PDT results
|
CR
|
PR
|
Total
|
Primary cancer
|
43 (91.5 %)
|
4 (8.5 %)
|
47 (100 %)
|
Recurrent cancer
|
34 (59.6 %)
|
23 (40.4 %)
|
57 (100 %)
|
TOTAL
|
77 (74 %)
|
27 (26 %)
|
104 (100 %)
|
CR – complete resorption; PR – partial resorption
With that, a total tumor resorption was observed in 77 patients (74 %), whereas 27 patients (26 %) showed a partial tumor resorption. A total resorption of primary tumors was up to 91.5 % (43 out of 47 patients), and of recurrent cancer – up to 59.6 % (34 out of 57 patients).
Due to the healing of a tissue defect after dissolution of a tumor by type of reparation, but not scarring, absolutely most patients have got a good cosmetic result.
In case of a partial resorption, small residual tumors were removed by means of high-frequency radio- and laser vaporization.
There was not any substantial difference in the efficiency of PDT depending on this or that type of a used photosensitizer. There was some difference regarding the frequency of side reactions and complications. In order of decreasing frequency of complications, the photosensitizers should be placed like this: Photolon, Photosense, Photohem, Radachlorin, Photoditazine, Foscan.
Table 2. PDT drug-light parameters
Photosensitizer
|
Drug dose,
mg/kg
|
Wavelength,
nm
|
Drug-light interval
(DLI), hours
|
Light dose,
J/cm2
|
Photohem
|
1.5 – 2.0
|
630
|
24 – 48
|
100 – 600
|
Photosense
|
0.5 – 1.5
|
675
|
24 – 72
|
100 – 600
|
Chlorin e6 derivatives
(Radachlorin, Photoditazine,
Photolon)
|
0.5 – 1.5
|
662
|
1 – 4
|
100 – 300
|
Foscan
|
0.04 – 0.15
|
662
|
24 – 96
|
40 – 100
|


Conclusion
The data we have got are convincing enough to estimate the PDT as a good alternative method of treatment for skin cancer localized on a face, aural cavities, the hairy part of a head, and on a neck, which makes it possible to achieve recovery with good and excellent cosmetic results in most patients.
Bibliography
- Christenson I.J., Borrowman T.A., Vachon C.M. et al. JAMA, 2005, 294 (6), pp.681-690.
- Cancer Facts and Figures, 2004, American Cancer Society.
- Malignant Tumors in Russia; 2005 (morbidity and mortality). Editors V.I.Chissov, V.V.Starinsky, G.V.Petrova. Moscow, 2006 (in Russian).
|
